INTRODUCTION
Stroke is a major global public health problem and it is the major cause of disability worldwide (Katan and Luft, 2018). Stroke is one of the main causes of mortality in adult populations of developed countries. In majority of the countries, stroke is the second or third cause of mortality (Ravichandran et al., 2019). Stroke survivors commonly have impaired motor control and balance that seriously affect their ability to lead an independent life and increasing burden to carers and society (Ravichandran and Janakiraman, 2016).
Basic trunk movement control is often impaired after stroke (Pappalardo et al., 2014). Malfunction of limb muscles in stroke is well documented, but little is known about the effect of stroke, in relation to trunk muscle activity. Unlike limb muscles, the innervation of trunk muscles is supplied from both cerebral hemispheres. The anterior corticospinal tract sends fibers mainly to the trunk or axial muscles. The control is both ipsilateral and contralateral. Therefore, trunk muscles are bilaterally cortically innervated (Karatas et al., 2004). Due to this reason, unilateral stroke could potentially deteriorate the function of trunk muscles on both the contralateral and ipsilateral sides of the body (Dickstein et al., 2000). In general, the trunk muscles are activated before the movement of upper and lower limbs. The initiation of trunk muscles is delayed in stroke subjects because the muscles involved in reach arm are activated earlier than the trunk muscles. Moreover, a comparison test using isokinetic dynamometer for analyzing the strength of trunk flexors, extensors, and rotators showed that stroke patients had statistically significant weaker trunk muscles than healthy people (Bohannon, 1992). In a patient with stroke, the importance of trunk control is often neglected (Van Criekinge et al., 2018).
Trunk control needs to be preceded in order to control limb movements and is correlated with functional movements (Hsieh et al., 2002). Activities of daily living (ADL) require trunk stability and mobility. Howe et al. (2005) confirmed that the impairment of trunk muscle after stroke limits ADL. Trunk control is a crucial component to perform ADL. Thus, trunk muscle performance is an important factor in predicting the functional outcome among stroke subjects. It is therefore necessary to identify the effective strategy to enable improvement in trunk balance and mobility among subjects with stroke.
Studies evaluating therapy aimed at improving trunk function are limited. Studies (Howe et al., 2005; Saeys et al., 2012; Verheyden et al., 2007) showed that trunk control ability can be improved by performing specific exercise training. Verheyden et al. (2009) suggested that trunk exercises performed in all planes in the supine position, improved the ability to control the trunk in subacute stroke patients. Ryerson et al. (2008) stated that proprioceptive training is essential to improve trunk control and balance. Most of the conventional trunk rehabilitation among stroke subjects is performed in stable surface. Few studies (Jung et al., 2016; Van Criekinge et al., 2018; Yoo et al., 2014) and supported implementation of an unstable surface in trunk rehabilitation among stroke subjects. These authors reported on articles that included air cushion, balance board, physioball, balance pads, and so on to simulate unstable surface. Physioball is unstable device presently permeates the fitness and rehabilitation environment. Generally, physioball exercise for trunk increases the need for force output from trunk muscles to provide adequate stability and balance. Limited studies are available in the literature examining physioball as an intervention in trunk rehabilitation among stroke subjects. There is no systematic review available in the literature to critically appraise the research evidence on performing trunk exercise with physioball in improving trunk performance among stroke subjects. Due to its common application in rehabilitation, conducting a systematic review on physioball among stroke subjects would validate its effectiveness in improving trunk performance. The objective of this study is to analyze the effectiveness of trunk exercise performed with physioball measured through trunk impairment scale as outcome tool in trials among stroke subjects.
MATERIALS AND METHODS
Eligibility criteria
This systematic review protocol was registered in the international database of prospective register of systematic reviews (PROSPERO), CRD42020135810 and was performed collectively by six authors (Ravichandran H, Janakiraman B, Gelaw AY, Gebremeskel BF, Haile TG, and Sharma HR). The review was conducted according to the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2015). Articles were selected according to the criteria mentioned below:
- Subjects with first onset, unilateral stroke.
- Minimum duration for onset of stroke is 10 days.
- Subjects aged 18–70 years.
- Both male and female genders.
- All randomized controlled trials, well-designed nonrandomized trials, and quasi-experimental designs intervening trunk exercise with physioball among stroke subjects.
- Articles using trunk impairment scale as outcome measure.
- Studies published in English and full-text availability.
- Studies were excluded if not having access to full test or articles published in languages other than English. Letters to the editor, comments, case reports, preclinical studies, and unpublished researches were also excluded.
Search strategy
Four authors (Ravichandran R, Janakiraman B, Gelaw AY, and Gebremeskel BF) conducted comprehensive search in January 2020, to identify articles published in databases such as PubMed, Cumulative Index and Nursing and Allied Health Literature (CINAHL), Physiotherapy Evidence Database (PEDro), and Google Scholar. The search was made using the following keywords or MeSH (medical subject heading) terms (if applicable); stroke or hemiplegia, and trunk stability or trunk balance, and physioball or Swiss ball or unstable surface, and trunk impairment or trunk impairment scale. Time restraints for the articles were set from 2009 and up to 2019. From 343 potentially appropriate articles, eight articles met the inclusion criteria of this review.
Study selection
Three authors (Janakiraman B, Haile TG, and Sharma HR) independently screened titles and abstracts to exclude articles out of scope. Eligible title and abstracts were retrieved for their full texts by two authors (Ravichandran H and Gelaw AY), to make selection decision according to the pre-established inclusion criteria. Any disagreements between the authors were resolved through consensus by discussing with author (Gebremeskel BF).
Hierarchy of evidence
Hierarchical system (Lloyd-Smith, 1997) was used to determine the level of evidence of included articles (Table 1). Two authors (Sharma HR and Gelaw AY) involved in this process and demonstrated that the articles included in this review had level of evidence ranged from 1b to 2b on hierarchy of evidence. In this study six randomized controlled trials, one nonrandomized controlled study and one quasi-experimental study design were included.
Data extraction
Three authors (Ravichandran H, Janakiraman B, and Gebremeskel BF) extracted data independently using a structured data extraction form adapted from Cochrane Back Review Group (van Tulder et al., 2003). Key data that were extracted includes the following items; general study information (title of the article, year of publication, first author’s last name, and geographical location of the study); design of the study and its characteristics (participant characteristics and outcome measures); outcome results with length of follow-up. Disagreements or conflicts during and after data extraction were resolved by a mutual agreement, and if needed, by requesting the opinion of the third reviewer (Haile TG).
Quality appraisal
All the authors independently evaluated the quality of included full-text articles, using quality assessment of controlled intervention studies tool developed by National Heart, Lung and Blood Institute (2014) of the National Institute of Health, United States. The quality of included articles was analyzed according to the 14 items listed in quality assessment of controlled intervention studies tool. One possible point was provided for each appraisal item if the included study fulfilled that item criteria. Based on the quality of included studies, the methodological quality assessed by this tool could range between 0 and 14. The methodological quality for each article was determined based their scores. Scores of 0 to 4 were considered as low grade, 5 to 10 as moderate grade and 11 to 14 as high grade. All the authors were consistent in performing quality assessment of included studies. Discrepancies or consensus among the authors were resolved by discussion with an expert. In this study, three RCTs with scores between 11 and 14 were considered as high grade in quality and five articles with scores between 5 and 10 were considered as moderate in quality. None of the included articles were low in quality (Table 2).
Risk of bias
Three authors (Ravichandran H, Gebremeskel BF, and Sharma HR) independently scrutinized the articles for potential risk of bias using the Cochrane Collaboration tool for risk of bias (Sterne et al., 2019). The domains formally assessed were sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias (Table 3).
Statistical analysis
Meta-analysis was performed using Cochrane’s Review Manager (RevMan) software (The Cochrane Collaboration, 2014). The effect sizes for continuous outcomes were expressed by mean difference in all trials. Mean difference with 95% confidence interval (CI) was used to determine changes in outcomes between physioball group and control group. This review considered a P-value of <0.05 to be statistically significant. The study by Nayak et al. (2012) was a single group quasi-experimental design and hence it was excluded from meta-analysis. Four separate meta-analysis were performed, using Trunk Impairment Scale and Brunnel Balance Assessment as the outcome measure: (a) effect size of physioball intervention in improving trunk performance during acute stage of stroke; (b) effect size of physioball intervention in improving trunk performance during subacute stage of stroke; (c) effect size of physioball intervention in improving trunk performance during chronic stage of stroke; (d) effect size of physioball intervention in improving balance among stroke survivors.
RESULTS
Study selection
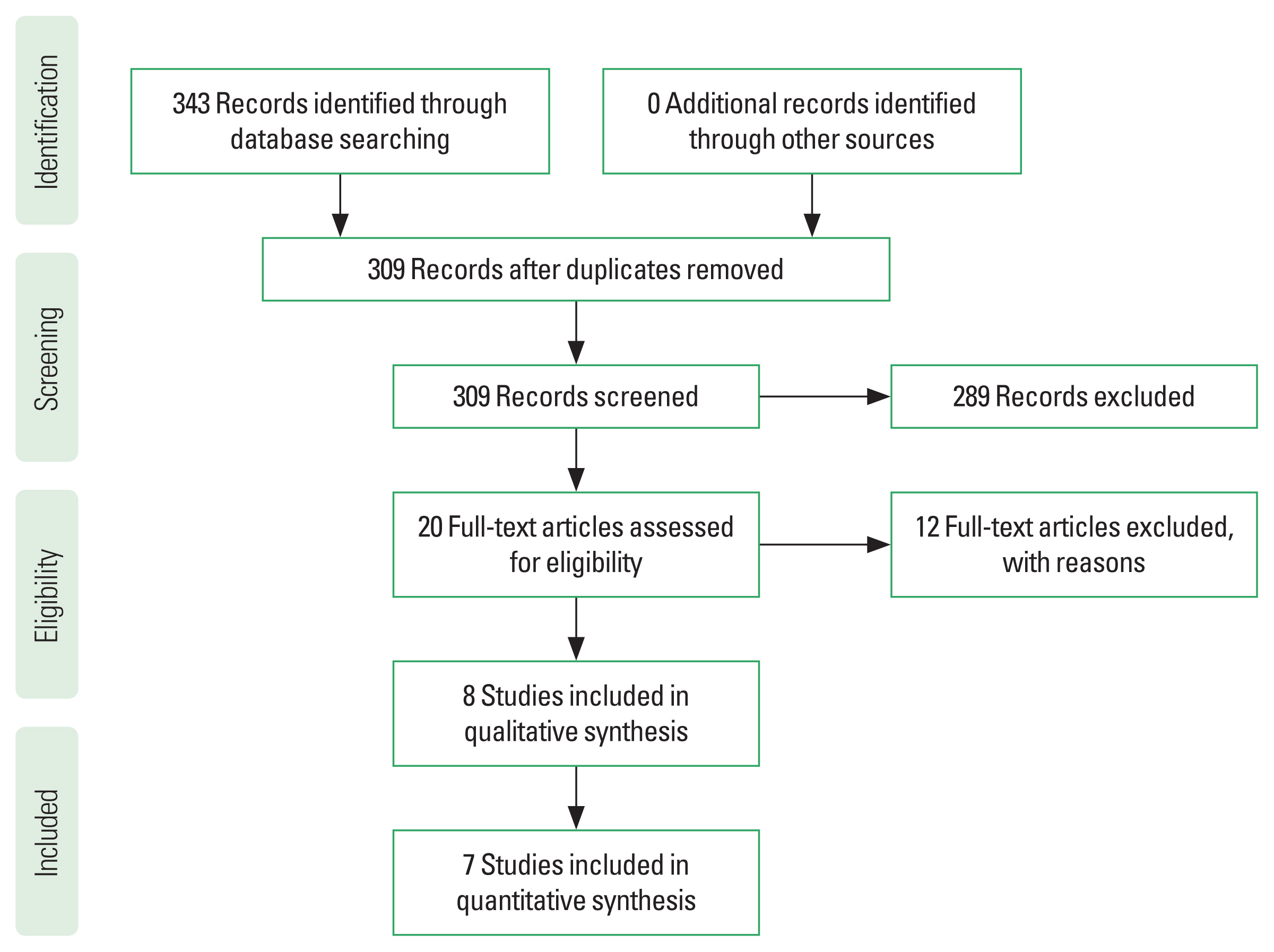
A total of 343 articles were identified in the initial search strategy. After the titles were screened, 34 articles were excluded as duplicates and 289 articles excluded because they did not meet the eligibility criteria. Of the 20 selected articles, 12 were excluded as they did not contemplate the objective of this review. Finally, eight articles were included in this review, out of which seven articles were included in the meta-analysis. The PRISMA flow diagram in Fig. 1 illustrates the study selection process.
Participants
Eight articles included a total of 273 participants, with 143 patients allocated to physioball intervention group and 130 participated in the comparative group. All studies included in this meta-analysis are from Asia and Europe. Mean age (standard deviation) of the participants included in the articles ranged between 49.2 (4.3) to 75.68 (9.4). The majority of participants were women. Ischaemic stroke was more prevalent among the participants and participants commonly affected on their right side of the body. Two articles have not reported the mean age, gender, causes of stroke, and side of body affected. Among the eight articles, 3 articles intervened among acute stroke subjects, 3 articles on subacute stroke subjects, and 2 articles performed with chronic stroke subjects. All the interventions were performed in hospital settings under the supervision of a therapist. The length of follow-up varied from 2 weeks to 12 weeks (Table 4). The mean quality of the included articles was 10 out of a total of 14 possible points. To determine the interrater reliability of authors Cohen Kappa was calculated (Kappa=0.83) and found to be almost perfect agreement.
Risk of bias within studies
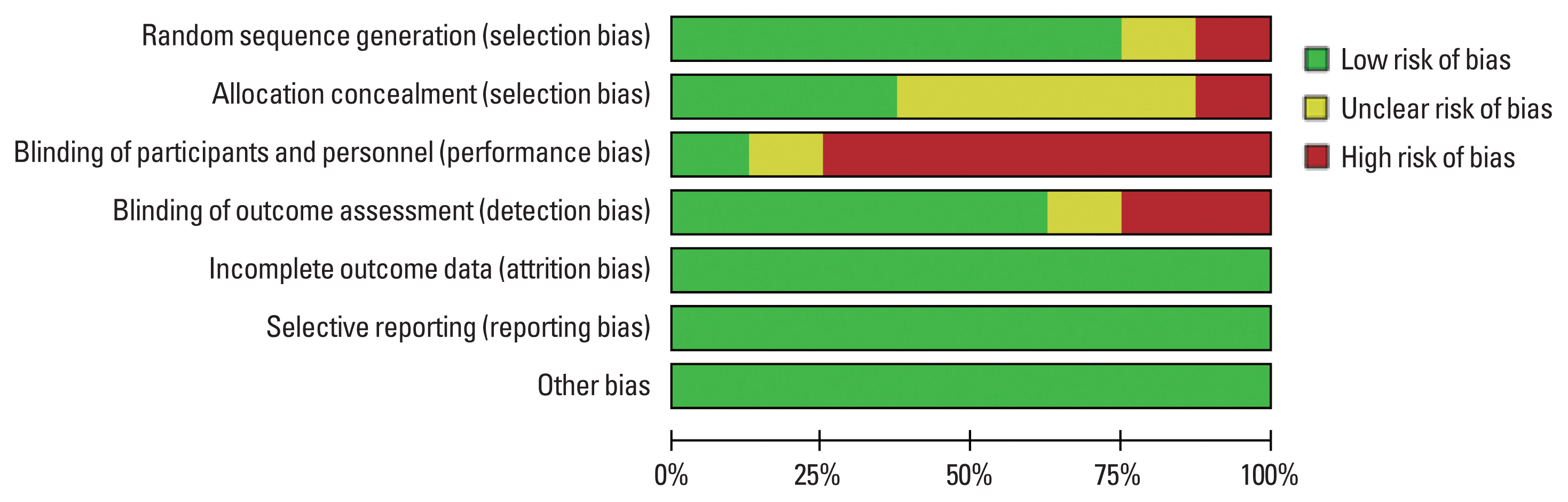
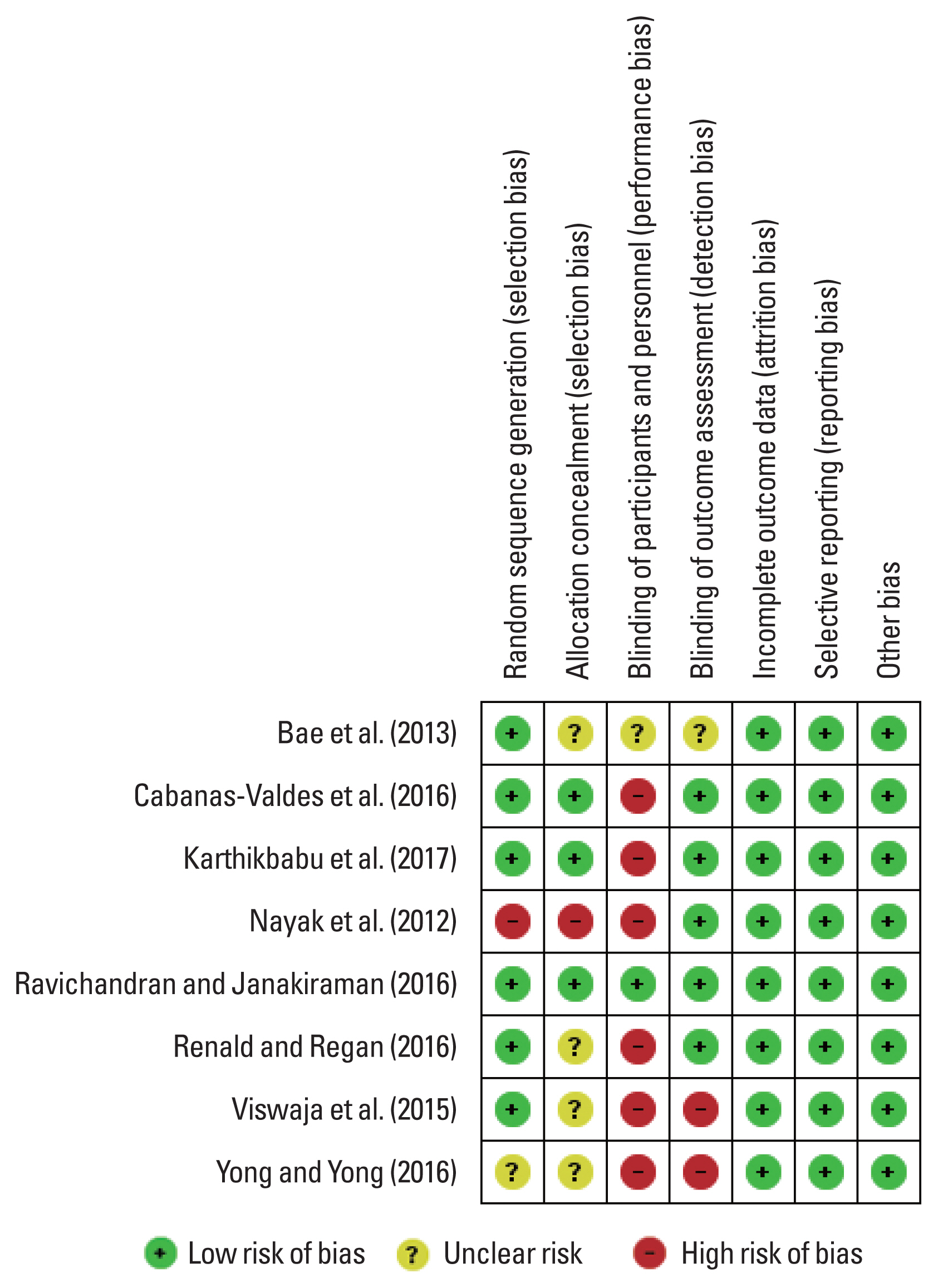
Randomization and allocation concealment demonstrated high risk in the quasi-experimental study performed by Nayak et al. (2012). Random sequence generation was reported in six articles and it was unclear in Seo and Oh (2016). Allocation concealment had low risk in three articles and was unclear in four articles (Bae et al., 2013; Renald and Regan, 2016; Seo and Oh, 2016; Viswaja et al., 2015). Blinding of participants was not performed in six studies and unclearly reported in one study. Outcome assessor was not blinded in two studies and unclear information was reported in one study. There was no incomplete data and selective reporting in the articles included and hence they had low risk. Ravichandran and Janakiraman (2016) had low risk in all the domains. The results of risk of bias were demonstrated in Figs. 2 and 3. The interrater Cohens Kappa statistics was 0.891.
Effect size of physioball intervention in improving trunk performance during acute stage of stroke
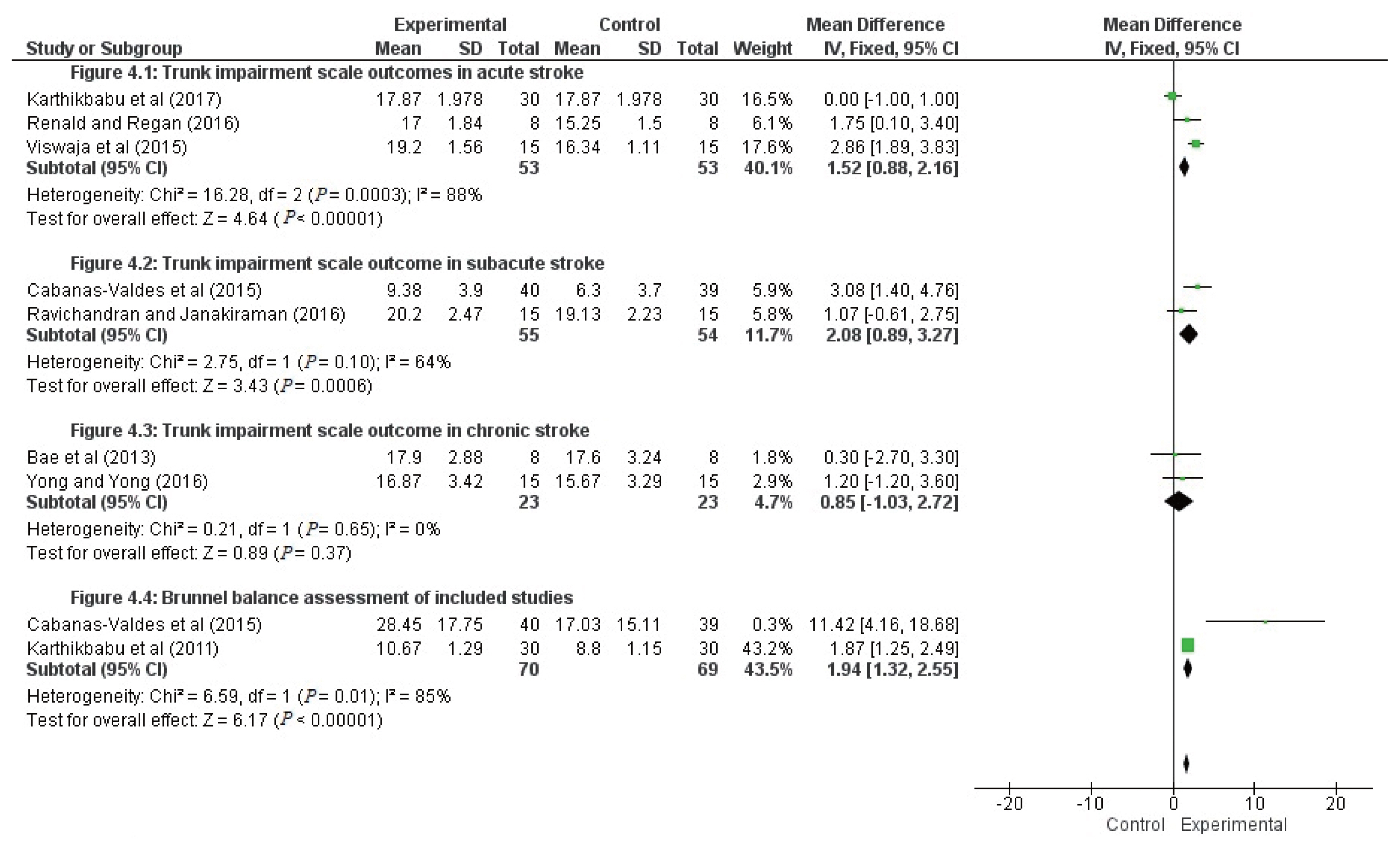
Three articles with 106 participants examined the trunk impairment scale outcome using physioball intervention during the acute stage (Fig. 4). The overall effect size (standardized mean difference) of 1.52 (95% CI, 0.88–2.16) suggests a large effect with high percentage of heterogeneity (88%). The study by Viswaja et al. (2015) with the largest treatment effect (2.86), reported a raw between-group effect size of 19.2. The other two studies, that favoring physioball intervention had large treatment effects of 0.00 and 1.75, respectively. Pooled estimation showed that physioball exercise is effective in improving trunk performance during the acute stage of stroke with P<0.00001.
Effect size of physioball intervention in improving trunk performance during subacute stage of stroke
Two studies investigated trunk impairment scale outcome using physioball intervention during the subacute stage among 109 participants. The pooled estimation resulted in a significant effect size of 2.08 (95% CI, 0.89–3.27) with moderate heterogeneity of I2= 64% (Fig. 4). Treatment effect was large (3.08) in the study by Cabanas-Valdés et al. (2016). Statistically significant P=0.0006 value favors that physioball exercise is effective in improving trunk impairment scale among subacute stroke patients.
Effect size of physioball intervention in improving trunk performance during chronic stage of stroke
Two studies investigating significance of physioball exercise in improving trunk impairment scale among 46 chronic stroke subjects were illustrated in Fig. 4. The overall effect size (standardized mean difference) of 0.85 (95% CI, −1.03 to 2.72) with low heterogeneity of 0%. Statistical result (P=0.37) of these two articles does not favor physioball exercise among chronic stroke subjects in improving trunk impairment scale outcomes.
Effect size of physioball intervention in improving balance among stroke survivors
The effect of physioball exercise in improving trunk balance was examined by pooling of data from Brunnel Balance Assessment from two studies involving 139 subjects. The overall effect size was 1.94 (95% CI, 1.32–2.55) with higher heterogeneity of 85% (Fig. 4). Statistically significant P-value of 0.00001 indicates that physioball exercise has a significant effect in improving balance of stoke subjects measured by Brunnel Balance Assessment.
Adverse effects
None of the eight articles included in this review have reported on adverse effects during or after the intervention. Cabanas-Valdés et al. (2016) reported death as a reason for excluding a control group participant in their randomized controlled trial.
Publication bias
Funnel plots were used to illustrate the risk of publication bias. The funnel plots for physioball exercise in improving trunk performance and balance among stroke survivors, resembles symmetrical, demonstrating a lower likelihood for publication bias. However, the results of funnel plots of this meta-analysis could be influenced by lower number of articles included in the literature. The authors suggest that this meta-analysis demonstrates a lower to moderate chances for publication bias.
DISCUSSION
This meta-analysis was performed to demonstrate the effects of physioball exercise in improving trunk performance among stroke subjects. There were no meta-analysis or systematic review performed in the past to evaluate the effectiveness of physioball in improving trunk performance among stroke subjects. To the best of our knowledge, this is the first meta-analysis to focus on the evidence concerning the effects of physioball exercise among stroke subjects.
Trunk impairment scale measuring the outcome of physioball exercise among stroke populations was set as an eligibility criterion to include article in this meta-analysis. Trunk impairment scale has been considered as a prediction instrument in the rehabilitation setting when considering the prognosis of stroke patients (Verheyden et al., 2007). There is variation in the type, intensity, and duration of physioball intervention implemented in the articles included for this review. The overall effect is good as demonstrated in the dynamic and coordination subscales of trunk impairment scale.
Articles included in this systematic review and meta-analysis demonstrated variance in comparison groups, intervention protocol, intervention duration, outcome measures, and quality of study. Heterogeneity rate was high in this meta-analysis due to small number of articles included and variance across the studies. The probable mechanism by which physioball could have worked is by facilitating the trunk control. Trunk exercise on the physioball poses a biomechanical demand on the trunk muscles. Postural perturbation experienced while exercising the trunk on the physioball is also another factor to facilitate trunk activity. Trunk exercise with physioball promotes anticipatory activation by maintaining the synergy between groups of muscles (Lehman et al., 2005). Exercising in a physioball facilitates postural control, trunk control, sitting, and dynamic balance control by maintaining interaction between nervous system, musculoskeletal system and contextual effects. These effects could not be achieved easily while exercising on the stable surface. The study results of Nagle (2011) also advocates on the positive effect of physioball exercises on the strength of abdominal and back muscles and balance to improve the performance for combat sports.
The result of this systematic review is similar to the previous review conducted by Behm et al. (2015). In that systematic review, 22 RCTs implementing unstable surfaces (Swiss ball, air cushion, balance board, and so on) for trunk training were included and their result concluded that unstable surface is effective in improving muscle strength, power and balance when compared to the controls. Recently another study, investigated the effect of trunk rehabilitation using unstable surfaces, on static and dynamic balance after stroke and with the evidence of seven RCTs, it concluded that trunk training on unstable support surface seemed to be superior to stable support surfaces in improving static and dynamic balance (Van Criekinge et al., 2018). These studies support the fact that unstable surface has beneficial effect in improving trunk performance.
Performing trunk exercise on a physioball is an area of concern needed in the literature. Trunk exercises performed with physioball is effective in improving trunk performance among hemiplegic subjects. More than improving trunk performance, physioball has the potential to facilitate upper limb and lower limb muscle cocontractions, which in turn improves the functional recovery following stroke. The results of this meta-analysis suggest that trunk exercise performed on the physioball has the potential to improve trunk performance for stroke survivors.
This meta-analysis provides insight into physioball exercises in improving trunk balance and stability for stroke subjects. The results of this meta-analysis emphasize the importance of focusing on stroke rehabilitation with unstable surfaces. First limitation of this study is there is limited availability of studies in the literature. Secondly, there exists a variance in diversity of stroke, side of stroke, and causes of stroke among the articles included in this meta-analysis. Thirdly, there exist differences in post interventional follow-up and lack of retention effect follow-up among the articles included in this review. Additionally, the authors could not able to trace the unpublished data or articles published in other language version to analyze the effect of publication bias.
CONCLUSIONS
The results of this study conclude that physioball exercise improves trunk performance and balance among subjects with stroke. Meta-analysis of included articles reveals that trunk improvement was significant during the acute and subacute stages of stroke. However, high percentage of heterogeneity suggests that more high quality randomized controlled trials with larger sample size in the future are required to justify this conclusion.