INTRODUCTION
Stroke has varying severity and subsequent functional impact, which depends on the recovery process of an individual and the extent of neurological damage (Chollet et al., 1991). Several stroke survivors experience physical, cognitive, perceptual, and mental impairments that require a period of intensive rehabilitation and may develop permanent disabilities (Teasell et al., 2005). Some stroke survivors can undergo a short period of inpatient rehabilitation program for recovery of function, and others continue to recover for a long period or throughout their lifetimes (Cramer, 2011). Therefore, in the intensive rehabilitation of individuals with neurological diseases, extremely important considerations must be made because of the reintegration of family and social roles and recreational activities (French et al., 2016; West and Bernhardt, 2012).
In rehabilitation settings, functional and task-specific trainings are the key elements of therapy and designed to assist stroke survivors in restoring their motor control to attain more-normal functional movement patterns (Teasell et al., 2005). Stroke survivors must have significant changes in the motor control and strength of the trunk and limbs, with an emphasis on the more-affected side and bilateral symmetric movement; these may be achieved using specific reeducation strategies (Veerbeek et al., 2014; West and Bernhardt, 2012). In terms of stroke rehabilitation settings, most previous studies were performed in laboratory or clinical settings that are less complex than the outdoor environment (Cho and Lee, 2013). Laboratory and clinical settings are not appropriate for establishing some complex personal space and community surroundings to meet the demands of multiple tasks for stroke survivors (Demain et al., 2013; Fung et al., 2012).
Virtual reality (VR) is a computer-generated environment that simulates a realistic experience for practicing functional tasks at intensities higher than those in traditional rehabilitation programs for stroke survivors (Chen et al., 2016). VR may help engage stroke survivors in a repetitive, intensive, and goal-oriented therapy to improve their functional disabilities, activity limitations, and participation restrictions, without considering the cost and burden associated with increasing the number of therapeutic sessions (Merians et al., 2002). Furthermore, VR provides real-time visual feedback for movements, thereby increasing engagement in enjoyable rehabilitation tasks. VR provides rehabilitative clinicians with new and effective therapeutic tools that can help treat various disabilities and enables remote therapy. VR-based interventions lead to clinical improvement and cortical reorganization through repetitive, adaptive, task-oriented, meaningful, and challenging exercises for stroke survivors (Laver et al., 2012).
As mentioned earlier, several virtual realities in rehabilitation interventions have been applied in the stroke population. However, the efficacy of VR rehabilitation interventions remains to be fully elucidated. In particular, studies on the qualitative and quantitative beneficial effects of VR on upper extremity function and independence in performing activities of daily living among patients with stroke are limited. The objectives of the present study were as follows: (a) to investigate the effectiveness of VR-based interventions in rehabilitation programs for restoring the upper extremity function of stroke survivors through a systematic review and (b) to examine the efficacy of VR-based interventions as part of a therapeutic rehabilitation program to improve upper limb function and independence in performing activities of daily living in stroke survivors by conducting a meta-analysis. Then, the VR-based interventions that are effective for improving upper limb function and independence in performing activities of daily living in stroke survivors were identified.
MATERIALS AND METHODS
Data sources and searches
A literature search of studies conducted between January 1, 2007, and August 31, 2017, was conducted using PubMed and EBSCOhost. The following key words were used: “hemiplegia” AND “virtual reality,” “hemiplegic” AND “virtual reality,” and “stroke” AND “virtual reality.” These terms were used as key words in the title and abstract of the studies in all databases. All the articles were cautiously screened by two reviewers, who selected relevant articles to be included in the present study.
Study selection
Studies that (a) were published in the English language; (b) involved adult patients with stroke; (c) included adult patients with hemiparesis after stroke during the acute, subacute, and chronic phases; (d) used randomized controlled trials; (e) investigated any form of immersive or nonimmersive VR-based interventions; and (f) used specific outcome measures to assess upper extremity function were included in the study. For the meta-analysis in this study, the inclusion criteria were as follows: First, the study aimed to improve upper extremity function after stroke using VR-based interventions. Second, the outcome measure was independence in performing activities of daily living. Third, the study must use validated and standardized evaluation tools with objective measurement units to determine the degree of independence in performing activities of daily living.
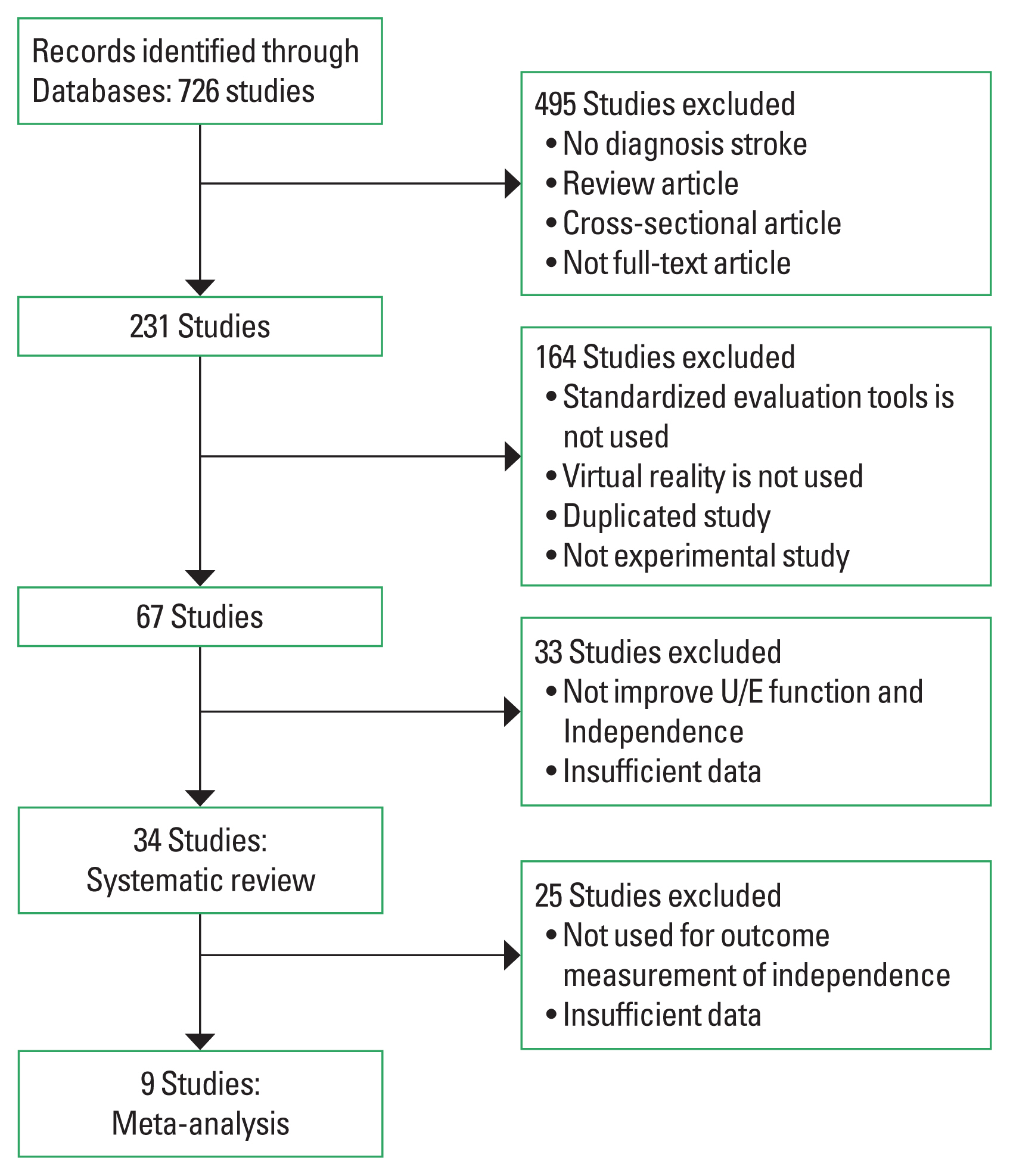
Two authors independently assessed the studies for eligibility. Any disagreement in the study selection was resolved during consensus meetings. By using this method, 726 articles were identified. Studies that were in accordance with the inclusion criteria or those that could not be included on the basis of the content of the abstract were selected for a full-text review. The abstracts of the remaining publications were evaluated for eligibility by two independent assessors. The systematic review method identified 726 studies, of which 692 had insufficient data required for the analysis. Thus, 34 articles were included in the systematic review by both assessors (Fig. 1).
Data extraction and quality assessments
The following data were extracted from the selected studies: diagnosis of the participants, age, study design, assessment, interventions, and operational definition. Finally, 34 studies were included. Nine studies were included in the meta-analysis. The following identifiable data were obtained from the studies: means and standard deviations, t-test results, and P-values (Table 1).
For the meta-analysis, the methodological quality of each study was assessed by two independent reviewers using the Jadad scale. The Jadad scale score was required for validating the quality of clinical trials, and blind raters assessed the quality to limit the risk of introducing bias into the meta-analyses and peer-review process. In addition, the nine articles were classified according to outcome measurements and the analysis of outcome measurements (Table 1).
Data synthesis and analysis
For the systematic review, the PICOS method was used to delineate the following five components of our literature review (Liberati et al., 2009): P (patient), adults who were diagnosed as having stroke; I (intervention), all types of VR-based interventions; C (comparison), rehabilitation intervention for a control group; and O (outcome), outcome measures for assessing upper extremity function and independence.
For the meta-analysis, Comprehensive Meta-Analysis version 2.0 (Biostat, Englewood, NJ, USA) was used to analyze the effect size, statistical heterogeneity, and publication bias in the selected studies. Effect size was calculated by dividing the ratio of the mean difference between the experimental and control groups by the standard deviation of the control group. The effect size for upper extremity function after stroke using VR-based interventions was determined using a standardized mean difference and 95% confidence intervals (CIs) in the fixed-effects model, which indicates the mean improvement in the standard scores of the experimental group relative to the control group.
Statistical heterogeneity refers to the degree of variation or inconsistency in the results of individual studies. Integrating research with different characteristics can lead to statistical heterogeneity and hence bias results; the heterogeneity of the studies was assessed using the Cochran Q test. Publication bias was assessed. A funnel plot and Egger regression interceptors were used. The funnel plot allows researchers to visually assess standard errors by reflecting the effect size on the horizontal axis.
RESULTS
Systematic review of studies
The study analyzed previous studies that evaluated the effects of VR-based interventions on upper extremity function after stroke. The 34 studies for systematic review included randomized controlled trials. A total of 1,507 patients with hemiplegic stroke were included. The mean number of participants was 678 in the VR-based intervention group and 829 in the control group. The experimental group consisted of a minimum of 5 participants and a maximum of 117 participants, whereas the control group had a minimum of 5 participants and a maximum of 268 participants.
The assessment tools used for the upper extremity functions were functional mobility assessment (FMA), Wolf motor function test (WMFT), and motor activity log (MAL). FMA was used in 23 studies; MAL, in 5 studies; and WMFT, in 5 studies. Meanwhile, the assessment tools used for assessing independence in performing activities of daily living were the Barthel index (BI) and functional independence measure (FIM). BI was used in 5 studies, and FIM was used in 4 studies (Table 2).
This study analyzed the types of VR interventions in 34 articles. The results are shown in Table 3. In terms of the VR-based interventions, VR systems that use computers, video games, and video capture and those with bilateral, goal-oriented, hand/arm, and reinforced feedback trainings were used in 20 studies. Six studies used games and Wii and Xbox, and two studies used robots. Furthermore, some studies used smart glove and smartphone programs, transcranial magnetic stimulation, RehabMaster, and the YouGrabber virtual system. On the basis of the results of this study, most VR-based interventions were related to upper extremity function and independence in performing activities of daily living in stroke patients.
Meta-analysis of the studies
The BI and FIM were used in the studies for meta-analysis, including 698 patients with hemiplegic stroke. The number of participants in each study ranged from 16 to 376. The methodological quality of the primary data was assessed using the Jadad scale score (Table 1). Three studies scored 1–4 of the maximum score of 4 points. The random assignments of the assessors were handled appropriately only in one study (Piron et al., 2010). Blinding of the assessors was properly addressed in three studies (Ballester et al., 2016; Choi et al., 2014; Shin et al., 2014). Data on all the patients and those who dropped out from the study were handled properly in seven studies (Ballester et al., 2016; Choi et al., 2014; da Silva Cameirão et al., 2011; Kiper et al., 2014; Piron et al., 2010; Shin et al., 2014; Zheng et al., 2015).
The overall effect size was moderate (0.41, P<0.001). The 95% CI ranged from 0.25 to 0.57 (Fig. 2). No significant heterogeneity and publication bias were found. Analysis of the funnel plot revealed the nine values that were to be distributed in every section, taking an asymmetric funnel shape, with more values falling on the right side of the mean effect size plot (Fig. 3).
In our test for statistical heterogeneity, a Cochran Q value of 21.78 (P<0.001) indicated no significant heterogeneity. The fixed-effects and random-effects models showed effect sizes of 0.41 and 0.65, respectively, providing further evidence of the lack of statistical heterogeneity among the studies included in the present meta-analysis (Tables 4, 5).
DISCUSSION
The present systematic review aimed to summarize interventions and outcome measurements after the use of VR technologies as interventions for improving upper extremity function and independence in performing activities of daily living in stroke survivors. Moreover, the effect of the VR intervention in the stroke patients was assessed in a meta-analysis.
In the 34 studies for systematic review, the assessment tools used for upper extremity functions were FMA, WMFT, and MAL. Meanwhile, the BI and FIM were used to assess for independence. Most of the applied interventions used VR using computer programs, followed by video games and Wii. Nine studies for meta-analysis used independence in activities of daily living as an outcome measure. The overall effect size of applying VR intervention in stroke survivors was 0.41, which is considered statistically significant. This result indicates that VR intervention has a moderate effect on improving upper extremity function and independence in activities of daily living. No significant heterogeneity and publication bias were identified. An adequate effect size was used for each study included in the meta-analysis. It may also have affected the results of the overall effect size because only few studies calculated the effect size in a meta-analysis.
In the 34 studies, the time and amount of therapy was similar between the VR-based intervention and control groups. In 18 studies, the participants in the experiment group received a VR-based intervention. Meanwhile, in the control group, the participants underwent the conventional rehabilitation program (Choi et al., 2014; Crosbie et al., 2012; da Silva Cameirão et al., 2011; Housman et al., 2009; Kiper et al., 2014; Lee et al., 2016a; Levin et al., 2012; Piron et al., 2010; Rand et al., 2014; Sin and Lee, 2013; Shin et al., 2014; Shin et al., 2015; Shin et al., 2016; Thielbar et al., 2014; Türkbey et al., 2017; Turolla et al., 2013; Yin et al., 2014; Zheng et al., 2015; Zondervan et al., 2016). In 16 studies, the control group received treatments similar or different from those used in the experiment group (Adie et al., 2017; Ballester et al., 2016; Broeren et al., 2008; Fluet et al., 2014; Kong et al., 2016; Lee et al., 2014; Lee et al., 2016a; Park and Park, 2016; Rand et al., 2017; Saposnik et al., 2010; Saposnik et al., 2016; Stockley et al., 2017; Subramanian et al., 2013; Viana et al., 2014; Zheng et al., 2015).
The results of this systematic review showed that VR intervention was more effective than the conventional therapy, as suggested by the significant improvements in upper limb function and independence in activities of daily living. For the assessment of upper extremity functions, FMA, WMFT, and MAL were commonly used, and BI and FIM were the most frequently used assessment tools for elucidating the effect of VR intervention on independence in activities of daily living. Although various VR-based rehabilitative interventions have been used in stroke patients, their efficacy in improving upper extremity function and independence in performing activities of daily living has not been fully elucidated. This study is unique because it examined upper extremity function and independence in performing activities of daily living. Our results showed that VR interventions may be effective for improving upper limb function and independence in performing activities of daily living in stroke patients.
In this study, only published articles obtained from the search process were reviewed, which may be a limitation because unpublished data and review papers or reports were excluded. Therefore, further studies that include a broader search for literatures on school-aged children must be conducted. Nevertheless, this study suggests various intervention methods that promote the development of cognitive function among children in the developmental stages. The cognitive function during the early stage of development is essential for the performance of children. Various cognitive approaches to rehabilitation therapy should be considered because it is an important skill in the preparation for learning (Cicerone et al., 2005). Furthermore, movements practiced in a virtual environment that closely mimic real-world tasks have been shown to maximize the effects of training (Chen et al., 2016; Laver et al., 2012). On the basis of previous studies, we investigated how VR intervention similar to real-world interventions affects upper limb function and independence in performing activities of daily living in stroke patients (da Silva Cameirão et al., 2011; Kiper et al., 2014; Shin et al., 2016). Training using intensive VR-based intervention has improved both upper and lower extremity functions and independence in performing activities of daily living in both the chronic and subacute populations (Chen et al., 2016; Lee et al., 2016b; Shin et al., 2016).
We cannot conclude whether VR-based interventions are more effective in promoting the recovery of independence in activities of daily living after stroke than any other approaches owing to the limited evidence from the meta-analysis. Nine studies for meta-analysis used variable VR-based intervention programs such as computer-, cellphone-, game-, and VR-based rehabilitation programs (Ballester et al., 2016; Choi et al., 2014; da Silva Cameirão et al., 2011; Kiper et al., 2014; Lee et al., 2016a; Piron et al., 2010; Shin et al., 2014; Turolla et al., 2013; Zheng et al., 2015). Moreover, the studies used various clinical measurement tools and were subject to methodological flaws. We suggest that these intervention factors affected the analysis of qualitative effects in this study. We also recommend that future studies should concentrate on investigating the effectiveness of clearly described individual techniques based on therapeutic methodology. For example, previous studies used small sample sizes; failed to include randomized controlled trials for experimenter bias, equivalence of participants, and co-interventions; and used poorly defined treatments and inappropriate outcome measures. The number of large-scale, multicenter randomized controlled trials that offer rehabilitative clinicians and stroke survivors a higher level of reliability is limited. Therefore, the important conclusions that can be drawn from these VR-based intervention studies are that collectively, we try to prove the consistent evidence of the beneficial effects of VR-based therapeutic interventions in comparison with those of other rehabilitation programs.
Finally, VR interventions may be beneficial to stroke patients, and we present the basis for the VR intervention applied in stroke patients by analyzing the intervention methods and type of outcome measurement. The number of VR interventions used in stroke patients may be significant. The study results can be used as a basis for the application of VR interventions in stroke patients in clinical settings.