INTRODUCTION
Cardiopulmonary exercise testing (CPET) has been used to evaluate the prognosis and risk stratification of pathological conditions in various heart diseases (Albouaini et al., 2007; Balady et al., 2010). The concept, methodology, and physiological basis have been well-established (Albouaini et al., 2007). To conduct effective exercise rehabilitation, the determination of adequate exercise intensity is essential. The workload at the ventilatory aerobic threshold (VAT) has been widely used to prescribe a reliable exercise intensity regimen (Mann et al., 2013).
Borg’s rating of perceived exertion (RPE) category ratio (CR) has been widely applied in prescribing exercise intensity for rehabilitation. Several studies have examined the relationship between Borg CR scales and CPET measurements at the VAT level (Zamuner et al., 2011). For the RPE that was analyzed according to the Borg CR-10 scale, the VAT points were close to a scale of 5 (“strong” perception) (Zamuner et al., 2011). On the CR-20 scale, a cohort study reported that a Borg CR of 11–14 corresponded with the lactate threshold (Scherr et al., 2013); meanwhile, values between 15–18 were considered above the threshold (Fletcher et al., 2013). The lactate anaerobic threshold closely coincided with Borg CR13 (somewhat hard) in healthy volunteers (Demello et al., 1987; Scherr et al., 2013). These reported findings showed a significant relationship between CR scales and CPET measurements, and Borg CR13 was reported to be closely identical to VAT.
Atrial fibrillation (AF), the most common sustained arrhythmia, has a significant impact on morbidity and mortality (Calkins et al., 2017). Catheter ablation is now widely applied for AF treatment, and the number of ablation methods is increasing (Kumagai et al., 2019; Nakatani et al., 2019; Yamaji et al., 2020). However, AF and atrial tachyarrhythmia (AT) recur in certain patients. Hence, AF/AT recurrence remains a major problem associated with AF ablation. Patients with AF are commonly old and have diabetes mellitus, hypertension, and other disorders affecting cardiac function. Many studies have demonstrated the importance of exercise in maintaining and improving cardiac performance (Anderson and Taylor, 2014; Shields et al., 2018). Self-monitoring and self-regulation of exercise intensity for exercise training are desirable and can be addressed using the Borg scale (Carvalho et al., 2009). AF patients during AF rhythm present with a variety of symptoms including palpitation, dyspnea, and chest discomfort (Levy et al., 1998). These patients are assumed to tolerate and adjust to their symptoms.
Based on these considerations, this study aimed to determine the association between the Borg CR scale and VAT in patients with AF after a successful ablation. We hypothesized that the workload at the Borg CR13 level on the CR 6–20 scale (Borg CR13-Watt) may not be similar to that observed at the VAT level (VAT-Watt) during CPET after AF ablation in AF patients who have achieved restored sinus rhythm (SR). Prior to this, no study has examined the relationship between Borg CR13-Watt and VAT-Watt in AF patients with restored SR after ablation.
MATERIALS AND METHODS
Patients
This was a single-center, retrospective study conducted at the Okayama Heart Clinic in Okayama, Japan. Inclusion criteria: patients with re-established SR after successful AF ablation. Exclusion criteria: patients with recurrent AF rhythm after ablation at the time of CPET. We performed CPET in 150 consecutive patients with restored SR (68±8 years; 45 females and 105 males) who underwent their first successful AF ablation between January 2018 and October 2021. This study aimed to examine the usefulness of Borg’s RPE CR scale in exercise prescription for patients with re-established SR after ablation using VAT-Watt as the control standard data. Consequently, we compared Borg CR13-Watt with VAT-Watt.
The sample size (n=150) had sufficient power to detect a difference of 15 watts by paired t-test (required minimal sample size was n=34, α=0.05, and power=0.80 for a difference of 10 watts and standard deviation of 20 watts). Similarly, the sample (n=150) had sufficient power to detect the correlation between Borg CR13-Watt and VAT-Watt (required minimal sample size was n=14, α=0.05, and power=0.80 for detecting a correlation coefficient of 0.70, β=0.20). The study was conducted in accordance with the principles of the Declaration of Helsinki 2000 and approved by the Institutional Ethics Committee of the Okayama Heart Clinic for Human Research (approval number, SN1). Written informed consent for the use of clinical data without personal information was obtained from all patients.
Ablation
The methods of PVI have been described in detail in another study (Yamaji et al., 2013). PVI was performed with the double LASSO technique using an electroanatomical integration mapping system (Ensite-NavX System, ABBOTT Japan, Tokyo, Japan). Ablation was performed using an open-irrigated ablation catheter (CoolFlexTM/FlexAbility, ABBOTT) via a steerable sheath. The PVI endpoint was defined as follows: (a) elimination of the PV potentials recorded by the two-ring catheters within the ipsilateral PVs and lack of left atrial (LA) capture during intra-PV, isthmus, and PV atrium pacing at least 30 min after the isolation and (b) no recurrence of PV spikes within all the PVs after an intravenous bolus administration of 20 to 40 mg of adenosine triphosphate during SR or coronary sinus pacing. With this, PVI was established.
Additional ablation in PVI was performed when required. This included the following: prophylactic cavotricuspid isthmus ablation, superior vena cava isolation, LA linear ablation, LA low-voltage area ablation, and ablation of complex fractionated atrial electrograms in the right and left atria. The decisions to select and perform these procedures were left to the discretion of the operator.
Cardiopulmonary exercise testing
All patients underwent symptom-limited CPET after AF ablation using a bicycle ergometer (StrangthErgo8, Mitsubishi Electric Engineering Co., Ltd., Tokyo, Japan). This was carried out at 101± 88 days (25th and 75th percentiles: 43 and 99 days) after the ablation. CPET testing was performed at 9:30–10:30 a.m. or 2:30–4:00 p.m. according to the scientific statement in a purpose-designed room (Balady et al., 2010). Using a bicycle ergometer, the exercise intensity was continuously increased by 5, 7, or 10 watts/min of the ramping up rate after 5, 7, and 10 watts, respectively, for a 4-min warm-up period. In addition to age, sex, and body weight, the program was dependent on the patient’s condition and planned to be completed within 8–12 min. The bicycle pedal rotation speed was set to 60 cycles/min. Minute ventilation, oxygen uptake (VO2), and carbon dioxide production were monitored continuously using a respiratory mass spectrometer with a breath-by-breath method (CPex1, OG Wellness, Okayama, Japan). The average of the moving VO2 for 8 sec was continuously calculated from the instantaneously detected VO2. Standard surface 12-lead electrocardiography was continuously performed (CardiMax8 FX-8800, Fukuda Denshi, Tokyo, Japan). The forearm blood pressure was determined every 15 min by the cuff oscillometric method with the Korotkoff Sound Technique (Tango M2, SunTach Medical, Morrisville, NC, USA). The termination criteria for CPET were as follows: (a) intolerance to exercise and (b) slowing down of the pedal rotation speed to 55 cycles/min by the patient.
The VAT points were determined by established methods (Balady et al., 2010; Beaver et al., 1986; Wasserman et al., 1973), and the workload at these points was obtained from the workload curve. Patients were asked about the subjective exercise intensity using a panel showing Borg 6–20 scales during CPET, and the patients pointed their fingers on the Borg scale board accordingly. The workload at Borg CR13 was also obtained from the workload curve.
Evaluation items
The following were analyzed: (a) a comparison of Borg CR13-Watt with VAT-Watt (ΔWatt), (b) examination of the relationship between ΔWatt and the duration from ablation to CPET, (c) regression analyses for Borg CR13-Watt versus VAT-Watt and Borg CR13-Watt versus ΔWatt, (d) evaluation of the agreement between Borg CR13-Watt and VAT-Watt using Bland–Altman plots, and (e) multivariate linear regression analysis to identify factors associated with ΔWatt.
Postablation care and follow-up and the definition of AT/AF recurrence
After discharge, the patients were followed up at our clinic at 2 weeks, 1 month, and 3 months. A telemetry electrocardiogram was recorded for 2 weeks after every follow-up to monitor symptomatic arrhythmias or to transfer the telemetry electrocardiogram once a day if asymptomatic. AT/AF recurrence was defined as any supraventricular tachycardia (AT and/or AF) lasting >30 sec and found 90 days (banking period) after the ablation.
Statistical analysis
Statistical analyses were performed using R ver. 3.2.2 (R Foundation for Statistical Computing, Vienna, Austria). The Kolmogorov–Smirnov test and histograms were used to assess the normal distribution of data. The Student t-test or Mann–Whitney U-test was used to compare the data between the two groups when appropriate. The homogeneity of variance was checked using the F-test. A Smirnov–Grubbs test was performed to detect outliers in each group’s data. Fisher exact tests with 2×2 tables and a two-tailed test for categorical variables were used to compare the two groups. Linear regression and correlation analyses were used to evaluate the relationships between Borg CR13-Watt and VAT-Watt as well as between Borg CR13-Watt and ΔWatt. The power analysis for paired comparison and correlation analysis were conducted using G*Power 3.1.9.7 (Faul et al., 2009). A Bland–Altman plot analysis was employed to assess the agreement between Borg CR13-Watt and VAT-Watt. We also performed multiple linear regression analyses to detect factors affecting ΔWatt. Given the relatively small number of patients, we used a stepwise method for the multivariate analyses. Furthermore, in the multivariate analysis, we initially chose 4–5 clinical factors, one echocardiographic factor, and factors of drug treatment in addition to age and sex. The analyses were performed repeatedly while changing the aforementioned factors. Afterwards, the final model was obtained. Data were expressed as mean±standard deviation. Differences were considered significant at P<0.05.
RESULTS
Patients’ characteristics
The clinical characteristics of the patients are summarized in Table 1. The data distribution of N-terminal prohormone of brain natriuretic peptide (NT-proBNP) was considerably skewed to the left and did not show a normal distribution pattern. The data for NT-proBNP were logarithmically transformed and presented with a normal distribution. Continuous variables for the other factors also showed a normal distribution pattern. No distinct data were observed among the clinical factors, echocardiographic parameters, and drug treatment.
Comparison between Borg CR 13-Watt and VAT-Watt
Analysis of mean and standard values
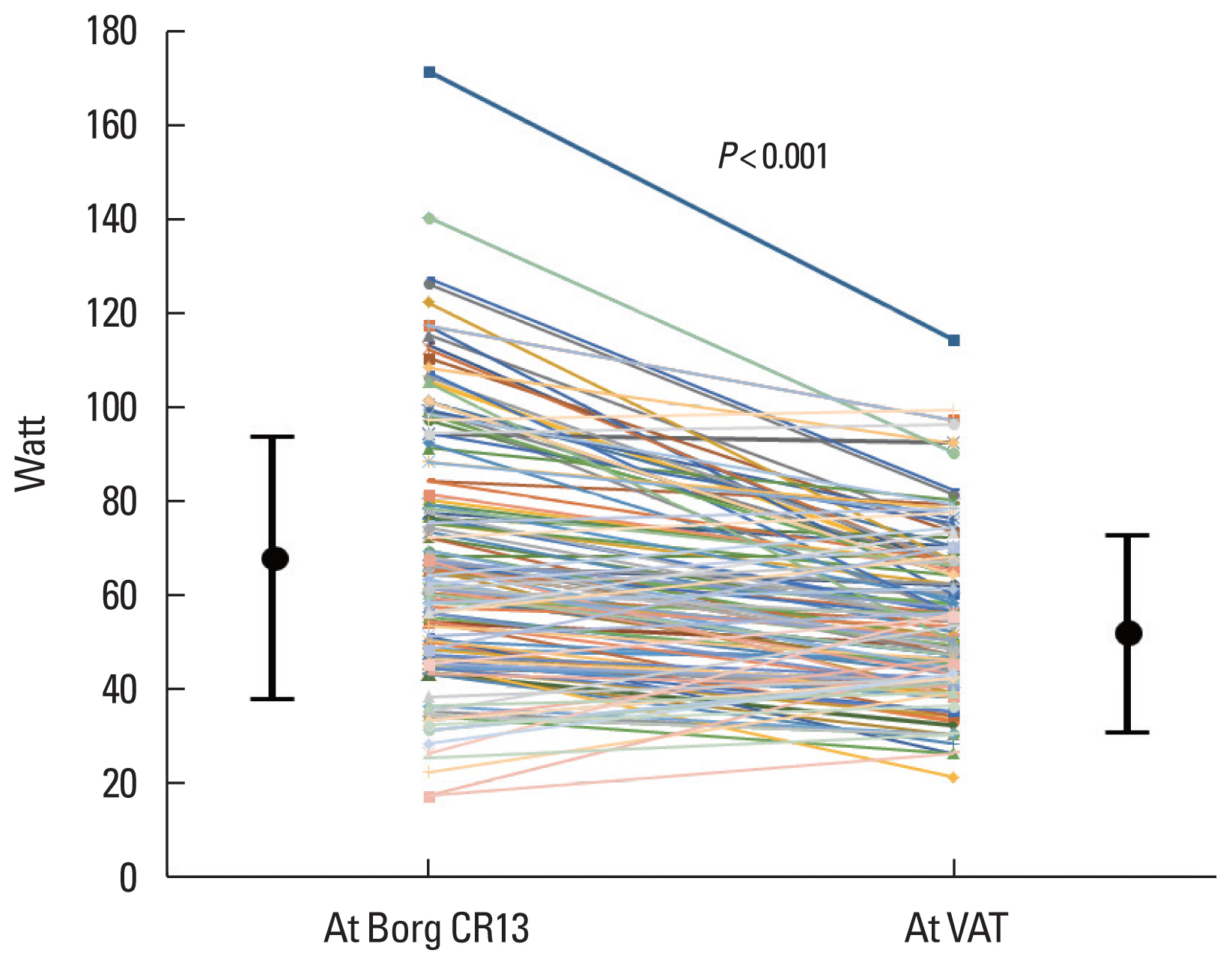
Fig. 1 shows the results of the comparison between Borg CR 13-Watt and VAT-Watt. Borg CR-13-Watt was significantly higher than VAT-Watt (67.2±27.8 vs. 54.7±17.6, P<0.01).
Bland–Altman plot analysis
The Bland–Altman plot is shown in Fig. 4. The Bland–Altman plot did not reveal that Borg CR13-Watt coincided with VAT-Watt. The difference between Borg CR13-Watt and the average of Borg CR13-Watt and VAT-Watt increased as the average of Borg CR13-Watt and VAT-Watt increased.
Clinical factors, drugs, and Watts
Relations of clinical and echocardiographic factors and drugs with Borg CR13-Watt, VAT-Watt, and ΔWatt are shown in Table 2. Although correlation analyses found a significant correlation between body height and weight, as well as body mass index, with respect to ΔWatt, the correlation coefficients were low. Male sex and use of antiarrhythmic drug treatment were significantly associated with a higher ΔWatt.
The results of the multivariate analyses are summarized in Table 3. Stepwise analyses using various combinations of independent factors finally showed that male sex and use of antiarrhythmic drugs were partially correlated with ΔWatt. These factors were also associated with a higher Borg CR13-Watt (Table 2). As noted above, a higher Borg CR13-Watt was associated with a higher VAT-Watt. These factors contributed to a higher ΔWatt through their association with a higher Borg CR13-Watt.
DISCUSSION
The main findings of this study were as follows: (a) Borg CR 13-Watt did not coincide with VAT-Watt in patients who achieved a successful AF ablation and (b) an increase in Borg CR13-Watt was associated with an increase in ΔWatt.
We performed CPET 101±88 days (25 and 75 percentiles: 43 and 99 days) after AF ablation, and no patient had AF/AT recurrence during CPET. AT/AF recurrence occurred in approximately 30% of patients within 3 months after ablation; the duration was defined as “the blanking period.” Early recurrence during the blanking period has been reported to predict late AT/AF recurrence (Themistoclakis and China, 2017). Mechanical injury, inflammation, and autonomic dysregulation were assumed to evoke early recurrences within the 3-month blanking period (Andrade et al., 2012). In the present study, CPET performed during the blanking period in approximately half of the patients was not associated with AT/AF recurrence in any patients. Furthermore, ΔWatt was not correlated with the duration between ablation and CPET, with a relatively low regression coefficient in the linear regression analysis. These results indicated that exercise itself did not affect AT/AF recurrence even during the blanking period in patients with successful ablation.
Borg CR13-Watt did not reflect VAT-Watt, and the results showed that the Borg scale by itself was not useful for prescribing exertion training intensity for patients with successful AF ablation. No study has examined the relationship between subjective symptoms determined using the Borg RPE scale and CPET measurements in these patients. Thus, the present results cannot be compared and discussed with previous reports. However, several reports have shown significant relationships between the two in healthy individuals and athletes (Garcin et al., 1999; Garnacho-Castano et al., 2018; Morishita et al., 2021; Zamuner et al., 2011). Furthermore, the Borg scale number at the VAT has been examined, and a Borg RPE CR of around 13 has been reported to coincide with the VAT workload (Demello et al., 1987). However, these reports were from studies on healthy volunteers. On the other hand, there have been reports that examined the relationship between the Borg scale and CPET parameters in patients with heart failure (Carvalho and Mezzani, 2011; Carvalho et al., 2009). These studies also showed that Borg RPE CR 11–13 is associated with VAT. A study found that Borg CR 11–13 was between the VAT and respiratory compensation points in patients with heart failure. The workload at the respiratory compensation point was higher than that found at the VAT. Hence, the workload at Borg CR 11–13 seemed to be higher than that at the VAT level. These results suggested that the Borg scales do not correspond sufficiently with the VAT. In this study, it was found that the workload at Borg CR13 did not coincide with the workload at the VAT level. Furthermore, Borg CR13-Watt was positively correlated with ΔWatt; hence, a higher Borg CR13-Watt was associated with a greater ΔWatt. Univariate and multivariate analyses suggested that male sex and the use of antiarrhythmic drugs contributed to an increase in ΔWatt. These factors may have contributed to the increase in Borg CR13-Watt and resulted in higher ΔWatt. Overall, this study indicated that the Borg scale alone was not useful for patients with re-established SR after AF ablation and suggested that the scale was not applicable for prescribing training intensity in individuals with pathological conditions.
This study did not primarily deal with the underlying mechanisms of differences between the workload at Borg CR-13 and the VAT. Symptoms in AF are well-known to vary considerably in each patient with a wide range of symptoms and substantively similar physiologies (Atarashi et al., 2008; Sears et al., 2005). Hence, relationships between symptoms in response to the physical load were estimated to be different between patients; that is, the Borg RPE CR scale to workload intensity was different among patients. In patients with successful ablation, it was still assumed that different subjective exercise feelings varied among patients. These may be the reasons for the inconsistency between the Borg RPE scale and the VAT in patients with AF ablation. With this, further discussion was not feasible due to the lack of relevant data.
This study had several limitations. First, this study selected Borg CR13 for analyzing the relationships between the Borg scale and VAT. However, Borg RPE CR12 or −14 was not examined. Workloads at Borg CR12 and −14 were higher and lower, respectively, as compared to those at Borg CR13. The present results revealed that the Borg CR13 workload itself was variable. Similarly, the workload at each Borg CR appears to be variable. The relationships between Borg CR12 or −14 and the VAT were highly presumed to show variable relationships between Borg CR-Watt and VAT-Watt. Second, the present study did not perform CPET before ablation. This study aimed to provide information on exercise prescriptions for patients with restored SR after ablation. Therefore, CPET before ablation appeared not to be required. Third, the present study did not examine healthy participants. The control standard values of the present study were VAT-Watt, which was compared with Borg CR13-Watt. In addition, many reports have examined the relationships between the Borg scale and aerobic threshold. Accordingly, the present study did not examine healthy persons. Finally, due to the varying circumstances of the patients, the duration of CPET after ablation could not be fixed. However, our results were confirmed by the noncorrelation of ΔWatt with the durations.
In conclusion, the Borg RPE scale was not identical to the VAT in patients with re-established SR after successful AF ablation. Higher Borg CR13-Watt was associated with a greater ΔWatt. When prescribing exercise training intensity for patients after AF ablation based on the Borg RPE scale, the Borg CR scale alone is not useful; hence, adjusting Borg CR13-Watt to fit VAT-Watt is necessary. Furthermore, CPET is recommended for patients in whom SR was re-established after AF ablation to precisely prescribe exercise intensity.