The effects of aquatic walking and jogging program on physical function and fall efficacy in patients with degenerative lumbar spinal stenosis
Article information
Abstract
The purpose of this study was to evaluate the effects of 12-week aqua walking and jogging program on muscle function, ankle range of motion (ROM), balance and fell efficacy in degenerative lumbar spinal stenosis (DLSS) patients. Six patients (2 males, 4 females) with DLSS participated in aquatic exercise program 3 times per week with each session of 60 min (warming-up, aqua walking, aqua jogging and cool down) at 1 m 20 cm–1 m 30 cm deep pool. Janda’s muscle function test, ankle ROM, Berg balance scale (BBS) and fall efficacy scale (FES) were analyzed before and after the training intervention. We found significant increases in balance, muscle function, ankle ROM and fall efficacy after training intervention. In conclusion, aquatic exercise seems to affect physical function and fall efficacy positively in elderly DLSS patients.
INTRODUCTION
As life expectancy increases, a larger number of patients suffer from lumbar spinal stenosis (LSS). The prevalence of lumbar spinal stenosis based on imaging criteria is estimated to be almost 50% in individuals older than age 60 (Boden et al., 1990; Kalichman et al., 2009). Degenerative lumbar stenosis (DLSS) shows bony overgrowth and ligament enlargement into the spinal canal (Yoshida et al., 1992) and diminished space available for the neural and vascular elements in the lumbar spine causes various symptoms (Kreiner et al., 2013). The symptoms include gluteal and lower extremity pain, numbness and motor weakness, which progressively get worsen by standing or walking and are alleviated by sitting (Genevay and Atlas, 2010; Kreiner et al., 2013). Therefore, LSS symptoms restrict walking capacity (Snyder et al., 2004) and increase the risk of falling (Kim et al., 2011).
Therapeutic exercises have shown to be effective in reduction of pain, improvement of disability, and increase of physical function among patients with chronic low back pain and LSS (Kim et al., 2014). Exercises for LSS patients often include unweighted walking or cycling, lumbar flexion exercises, hip mobility exercises and core strengthening (Backstrom et al., 2011; Iwamoto et al., 2010). However, to train with unweighted walking for LSS, particular machine is needed and it can be limitedly applied to LSS patients.
The upward thrust exerted by water on a body virtually eliminates the effects of gravity and the body’s buoyancy reduces compression on the lower back, allowing for more pain free movement (Kaneda et al., 2007). Up to now, numerous studies have demonstrated that aquatic exercise has various advantages for elderly people. However, very few data exist on the physiological effect of aqua exercise on the DLSS patients. Therefore, we examined the effects of 12-week aqua walking and jogging program on muscle function, range of motion (ROM) of ankle, balance and fell efficacy in DLSS patients.
MATERIALS AND METHODS
Subjects
6 subjects (2 males, 4 females) with DLSS participated in the study (Table 1). They had previously been screened and diagnosed by an orthopedic surgeon. They had not been getting active treatments; none of them had surgery before and were currently not performing training. The subjects didn’t present any neurological signs of pathological importance in the clinical examination. Prior to the study, participants were informed about the purpose, procedures and risks of the study and written informed consent was obtained from each participant.

Physical characteristics of subjects
Aquatic exercise program
Subjects participated in aquatic exercise program 3 times per week with each session of 60 min at 1 m 20 cm–1 m 30 cm deep pool. The program was composed of warming-up (10 min), aqua walking (20 min), aqua jogging (20 min), and cool down (10 min).
Janda’s muscle function test
Janda’s muscle function test was developed (Janda, 1983) for muscles responsible for movement in the face, trunk, upper limb and lower limb. Through this test, shortened muscles for limited joint movements and hypermobile joints can be identified. At the start of each subsection, the relevant joint movements, muscle and nerve supply were explained and proper test position was demonstrated to the subjects. In each test, muscle function was assessed with regard to a 6 point scale, which ranges between normal function (score 0) and complete shortness or contracture (score 6).
ROM of ankle
Subjects lay supine with outstretched legs on an examination table without any pad, cushion or pillow underneath. The testing position of ankle started 90° and the ROM of the ankle was calculated by the summation of degrees of plantar flexion and dorsi flexion. The greater degree means the higher flexibility.
Berg balance scale (BBS)
The BBS was developed (Jogi et al., 2011) as a performance-oriented measure of balance in elderly individuals. The BBS consists of 14 items that are scored on a scale of 0 to 4. A score of 0 is given if the participant is unable to do the task, and a score of 4 is given if the participant is able to complete the task based on the criterion that has been assigned to it. The maximum total score on the test is 56.
Fall efficacy scale (FES)
FES was developed by Azad et al. (2014) and is a questionnaire composed of 16 items of simple mobility tasks and more difficult tasks including the 10 original items and six new items assessing walking on slippery, uneven or sloping surfaces, and visiting friends or relatives, going to a social event or going to a place with crowds. We used the revised FES instructions and response categories that assess level of concern about falling when carrying out each activity on a four point scale (1=not at all concerned, 4=very concerned).
Statistical analysis
Data are presented as mean values with SD. A paired t-test was used to evaluate differences between before and after training. SPSS software (SPSS for Windows, version 22.0, Chicago, IL, USA) was used for all analyses, and a P-value of 0.05 was set for significance.
RESULTS
Muscle function and ankle flexibility
The scores of Janda’s muscle function tests were significantly decreased after exercise program in back muscle and lower body muscles except abductor of thigh. however, pectoralis major and neck muscle didn’t show any change between pre and post exercise. Ankle ROM was also significantly increased from 53.8±11.8° to 68.8±8.6° (Table 2).
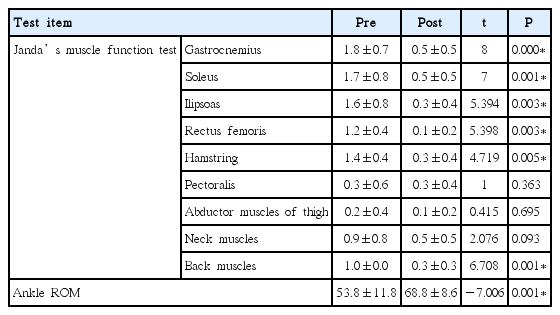
The change of score of muscle function test and ankle ROM
Fall efficacy and balance
After 12 week program, the scores of BBS and FES were significantly increased from 27.2±4.9 to 34.7±3.3 and 73.0±21.4 to 98.8±2.4, respectively. It means that aquatic exercise program affected the function of balance and confidence of not falling positively in the patients with stenosis (Table 3).

The change of BBS and FES
DISCUSSION
DLSS can cause decreased strength, balance and impaired gait pattern (ECRI Health Technology Assessment Group, 2001) and overall stiffness (Backstrom, 2011). One of the common symptoms of LSS is neurogenic claudication which progressively get worsen by standing or walking and are alleviated by sitting (Genevay and Atlas, 2010; Kreiner et al., 2013). Therefore, Individuals with LSS commonly show the reduced walking tolerance (Onel et al., 1993) and have a risk of a fall comparable with the patients of degenerative knee osteoarthritis (Kim et al., 2011).
To decrease the risk of falling by improving physical function in DLSS patients, aquatic walking and jogging program was executed in our study. Water supplied safe environment to the patients having ambulation problem and permitted them upright exercise. As a result, 12 week aquatic exercise showed positive effects such as increases of balance, muscle function, ankle ROM and fall efficacy in elderly DLSS patients. Many other studies have demonstrated that water exercise is effective in increasing muscle strength, flexibility, balance and fall efficacy in elderly people (Fisken et al., 2015; Kim and O’Sullivan, 2013; Sato et al., 2011). The combined properties of hydrostatic pressure and viscosity of water provide favorable conditions for resistance and proprioceptive training. These features of water might have acted positively to improve balance, muscle function and flexibility. And another reason for improvement of physical function is exercise itself. The buoyancy of water can relieve the limitation of the movement by pain and fear of falling of LSS patients. It permitted them relatively active movements. The improvements of balance, muscle function and ankle ROM might have affected the increase of fall efficacy positively because balance deficit and muscle weakness are main risk factors for falling (Rubenstein, 2006; Rubenstein and Josephson, 2006) and ankle is the important body part for the strategy of keeping balance and avoiding falling (Winter, 1995).
In the absence of a control group, we can only surmise that the results in our study were probably a combination of the effect of intervention and the natural course of DLSS. Further researches are needed to verify current results and draw conclusions regarding independent effectiveness of aquatic exercise as a treatment for DLSS.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.