Efficacy of conservative treatment on exacerbation of adolescent idiopathic scoliosis
Article information

Abstract
Scoliosis is defined as a deviation from the normal vertical line of the spine and consists of a lateral curvature in which the spine rotates within the curvature. Adolescent idiopathic scoliosis (AIS) is the most common form of scoliosis and the cause is unknown. In this study, it was investigated whether conservative treatment for adolescent idiopathic scoliosis (CONTRAIS) reduced the patient’s Cobb angle, and the effect of CONTRAIS according to the severity of idiopathic scoliosis and the efficacy of CONTRAIS by spinal region were also verified. Idiopathic scoliosis patients with a Cobb angle of 10° or more were recruited and classified into mild, moderate, and severe groups according to the Cobb angle (°). Cobb angle was measured radiographically before and after 10 weeks of treatment. A combination of CONTRAIS, including physical therapy, exercise therapy, manual therapy, and home exercise was prescribed for all patients. The patients visited the hospital 3 times a week for 10 weeks for treatment, and exercised at home for 20 min every day. In this study, the effect of reducing Cobb angle of CONTRAIS did not differ according to the spinal region. Also, the Cobb angle reduction effect of CONTRAIS was more effective in severe group. This study may suggest that early detection and treatment through CONTRAIS enables successful correction of AIS.
INTRODUCTION
Scoliosis is defined as a deviation from normal vertical line of the spine and consists of a lateral curvature with rotation of the spine within the curve. A typical case of scoliosis involves at least 10° of spinal curvature on posterioranterior radiographs involving spinal rotation. Scoliosis affects 0.2%–6% of the population and is diagnosed as idiopathic scoliosis (IS) in 70% of structural malformations affecting the spine in children and adolescents. Spinal malformations are the most common orthopedic malformations in children and adolescents (Dayer et al., 2013; Trobisch et al., 2010). However, although previous studies have investigated the clinical variables for the onset, curvature progression, severity related to clinical prognosis, and current treatment modalities, the causes of IS have not been adequately identified (Yaman and Dalbayrak, 2014).
Adolescent idiopathic scoliosis (AIS) is the most common form of scoliosis and the cause is unknown. AIS is found in people aged 10 years and older and is defined as a curve measuring at least 10° (Cobb angle measured on x-rays) (Choudhry et al., 2016). People with AIS are usually asymptomatic, but the resulting surface anomalies can negatively affect adolescent patients. Additionally, increased curvature of the spine may pose health risks in adulthood (Sud and Tsirikos, 2013). In order to maximize the effect of treatment, the degree of curvature, the affected area, the balance of the trunk, overall health, function and satisfaction, and the treatment needs of patients and parents are should be satisfied (Motyer et al., 2021; Wong and Tan, 2010). In general, surgery is recommended for curves greater than 40° to 50° to prevent progression of the curve (Addai et al., 2020). However, long-term follow-up is lacking and does not draw meaningful conclusions (Kuznia et al., 2020). Bracing is defined as the application of external supports to the trunk and is usually rigid and applied to achieve maximum correction of the pathological curve. This treatment is started when the curve is diagnosed as progressive or exceeds the 30° Cobb angle. In general, braces must be worn for a significant amount of time per day over several years until bone growth is complete, which typically occurs at age 16 in girls and 18 in boys (Schiller et al., 2010). This can have a serious negative impact on the quality of life of children and adolescents. physical therapy (PT) consists of individually coordinated exercises for the patient in a center dedicated to the treatment of scoliosis. PT has potential benefits for treating physiological and psychological aspects of patients with AIS (Ceballos Laita et al., 2018; Zhou et al., 2021). Conservative interventions in adolescents with IS remain controversial (Anthony et al., 2021; Bettany-Saltikov et al., 2017). Despite numerous reviews published, there is no clear methodological evaluation of the paper.
The goals of AIS surgery are to stop the progression of the curve, correct the deformity, maintain a balanced spine in the coronal and sagittal planes, preserve as many movable vertebral segments as possible, and prevent surgical complications (Fischer and Kim, 2011). However, despite the benefits of surgical strategies for AIS, there is insufficient evidence that surgery is superior to nonsurgical interventions in patients with severe AIS. This means that there is no convincing evidence that certain types of treatment for AIS are superior to others (Bettany-Saltikov et al., 2016). Brace has been the mainstream nonsurgical treatment for AIS for the past 50 years. In addition to braces, many other treatments have been tried (such as electrical stimulation, biofeedback, manual therapy [MT], PT, and exercise) (Schiller et al., 2010). Successful orthotic care requires a high level of involvement with AIS patients and their support networks: parents, family, friends, orthopedic surgeons, and orthosis specialists. Poor adherence to brace patient wearing schedules is another obstacle to successful orthosis management (Meng et al., 2017).
CONTRAIS comprises braces, scoliosis-specific exercises, MT, and electrical stimulation. Interestingly, very positive results of CONTRAIS have been reported (Ceballos Laita et al., 2018; Zhou et al., 2021). However, nonsurgical interventions for AIS are controversial (Day et al., 2019; Fan et al., 2020). Previous studies have suggested that nonsurgical therapy is an effective treatment for scoliosis, particularly AIS (Dufvenberg et al., 2021; Ng et al., 2017). However, the prevalence of scoliosis is increasing, and many researchers argue that current treatments for AIS are insufficient (Cheung et al., 2020; Płaszewski and Bettany-Saltikov, 2014).
In this study, it was investigated whether CONTRAIS reduces the Cobb angle of the AIS patient. The effect of CONTRAIS according to the severity of IS and the efficacy of CONTRAIS for each spinal region were verified.
MATERIALS AND METHODS
Composition of CONTRAIS
In this study, 157 adolescent IS patients out of 326 IS patients from an orthopedic hospital in Seoul were selected. A combination of CONTRAIS including (PT), exercise therapy (ET), MT, and home exercise (HE) was prescribed for all patients. Patient treatment (PT, ET, MT) for IS was performed twice a week at the hospital for 10 weeks, and during the treatment period, HE was performed for 20 min a day, 3 times a week (Table 1). The composition of HE is shown in Fig. 1.

Clinical program for CONTRAIS
Composition of home exercise.
Patients
Patients with IS with a Cobb angle greater than 10 degrees were recruited and classified according to the Cobb angle (degrees) as mild group (n=47, 10º ≤ Cobb angle ≤25), moderate group (n= 38, 25º< Cobb angle ≤40º), and severe group (n=72, Cobb angle >40º). All patients with AIS included 131 women (83.4%) and 26 men (16.6%), and the ages ranged from 10 to 18 years (Table 2).

Patient's demographics
Research design
This study was a treatment process for patients (Clinical trial number: KSH-2021-001), and the procedure was conducted as an observational study in a retrospective controlled cohort and serial outpatients. Cobb angle was measured radiologically by an orthopedic surgeon with expertise in IS. Radiologic measurements were performed before and after 10 weeks of treatment. For the evaluation of IS, changes in Cobb angle were measured by digital radiography x-ray before and after CONTRAIS, and changes in appearance were observed using global posture system (Fig. 2). PT performed transcutaneous electrical nerve stimulation, radiofrequency and extracorporeal shock wave therapy for the patients. At the same time, ET, MT, and HE were treated for 10 weeks. The patients visited the hospital 3 times a week for 10 weeks and received treatment, and they exercised at home for 20 min every day using a HE sheet guided by an orthopedic surgeon. All patients were prescribed 20 min of HE and interviewed at each visit to check whether they were doing HE.

Cobb angle and global posture system measurement before and after CONTRAIS. CONTRAIS, conservative treatment for adolescent idiopathic scoliosis.
Statistical analysis
All statistical analyzes were performed using IBM SPSS Statistics ver. 28.0 (IBM Co., Armonk, NY, USA). Student t-test was applied to compare changes in CONTRAIS treatment, and the significance level was set to P<0.05.
RESULTS
Table 3 shows the changes in Cobb angles before and after CONTRAIS treatment for AIS patients.
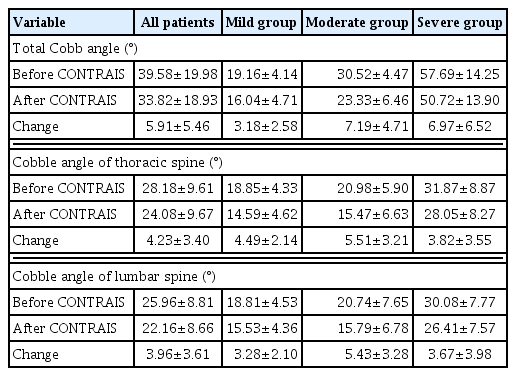
Mean changes of Cobb angles before and after CONTRAIS treatment
Effects of CONTRAIS on Cobb angles in all AIS patients
The Cobb angles before and after CONTRAIS were compared in all patient. The total Cobb angle of thoracic and lumbar spine decreased from 39.58±19.98 before CONTRAIS to 33.82±18.93 after CONTRAIS, and the difference (5.91±5.46) was statistically significant from Student t-test (P<0.001). The Cobb angles of the thoracic spine before and after CONTRAIS were compared in all patients. The Cobb angle of the thoracic spine decreased from 28.18±9.61 before CONTRAIS to 24.08±9.67 after CONTRAIS, and the difference (4.23±3.40) was statistically significant from Student t-test (P<0.001). The Cobb angles of the lumbar spine before and after CONTRAIS were compared in all patients. The Cobb angle of the lumbar spine decreased from 25.96±8.81 before CONTRAIS to 22.16±8.66 after CONTRAIS, and the difference (3.96±3.61) was statistically significant from Student t-test (P<0.001). Based on these results, CONTRAIS was found to be effective for reducing Cobb angles of the total, thoracic spine, and lumbar spine in all AIS patients (Fig. 3).
Cobb angles before and after CONTRAIS in all adolescent idiopathic scoliosis patients. CONTRAIS, conservative treatment for adolescent idiopathic scoliosis; T-spine, thoracic spine; L-spine, lumbar spine. ***P<0.001.
Effects of CONTRAIS on Cobb angles in the mild group
The Cobb angles before and after CONTRAIS in the mild group were compared. The total Cobb angle of thoracic and lumbar spine decreased from 19.16±4.14 before treatment to 16.04±4.71 after treatment, and the difference (3.18±2.58) was statistically significant from Student t-test (P<0.001). The Cobb angles of the thoracic spine before and after CONTRAIS were compared in the mild group. The Cobb angle of the thoracic spine decreased from 18.85±4.33 before CONTRAIS to 14.59±4.62 after CONTRAIS, and the difference (4.49±2.14) was statistically significant from Student t-test (P<0.001). The Cobb angles of the lumbar spine before and after CONTRAIS were compared in the mild group. The Cobb angles of the lumbar spine decreased from 18.81±4.53 before CONTRAIS to 15.53±4.36 after CONTRAIS, and the difference (3.28±2.10) was statistically significant from Student t-test (P<0.001). Based on these results, CONTRAIS was found to be effective for reducing Cobb angles of the total, thoracic spine, and lumbar spine in the mild group of AIS patients (Fig. 4)

Cobb angles before and after CONTRAIS in the mild group. CONTRAIS, conservative treatment for adolescent idiopathic scoliosis; T-spine, thoracic spine; L-spine, lumbar spine. **P<0.001.
Effects of CONTRAIS on Cobb angles in the moderate group
The Cobb angles before and after CONTRAIS in the moderate group were compared. The total Cobb angles of thoracic and lumbar spine decreased from 30.52±4.47 before CONTRAIS to 23.33±6.46 after CONTRAIS, and the difference (7.19±4.71) was statistically significant from Student t-test (P<0.001). The Cobb angles of the thoracic spine before and after CONTRAIS were compared in the moderate group. The Cobb angles of the thoracic spine decreased from 20.98±5.90 before CONTRAIS to 15.47±6.63 after CONTRAIS, and the difference (5.51±3.21) was statistically significant from Student t-test (P<0.001). The Cobb angles of the lumbar spine before and after CONTRAIS were compared in the moderate group. The Cobb angles of the lumbar spine decreased from 20.74±7.65 before CONTRAIS to 15.79±6.78 after CONTRAIS, the difference (5.43±3.28) was statistically significant from Student t-test (P<0.001). Based on these results, CONTRAIS was found to be effective for reducing Cobb angles of the total, thoracic spine, and lumbar spine in the moderate group of AIS patients (Fig. 5).
Cobb angles before and after CONTRAIS in the moderate group. CONTRAIS, conservative treatment for adolescent idiopathic scoliosis; T-spine, thoracic spine; L-spine, lumbar spine. ***P<0.001.
Effects of CONTRAIS on Cobb angles in the severe group
The Cobb angles before and after CONTRAIS in the severe group were compared. The total Cobb angles of thoracic and lumbar spine decreased from 57.69±14.25 before CONTRAIS to 50.72±13.90 after CONTRAIS, and the difference (6.97±6.52) was statistically significant from Student t-test (P<0.001). The Cobb angles of the thoracic spine before and after CONTRAIS were compared in the severe group. The Cobb angles of the thoracic spine decreased from 31.87±8.87 before CONTRAIS to 28.05±8.27 after CONTRAIS, and the difference (3.82±3.55) was statistically significant from Student t-test (P<0.001). The Cobb angles of the lumbar spine before and after CONTRAIS were compared in the severe group. The Cobb angles of the lumbar spine decreased from 30.08±7.77 before CONTRAIS to 26.41±7.57 after CONTRAIS, and the difference (3.67±3.98) was statistically significant from Student t-test (P<0.001). Based on these results, CONTRAIS was found to be effective for reducing Cobb angles of the total, thoracic spine, and lumbar spine in the severe group of AIS patients (Fig. 6)
Cobb angles before and after CONTRAIS in the severe group. CONTRAIS, conservative treatment for adolescent idiopathic scoliosis; T-spine, thoracic spine; L-spine, lumbar spine. ***P<0.001.
CONTRAIS effects on Cobb angles among the treatment groups
Next, analysis was conducted focusing on the change of Cobb angle for the patient group according to the severity of the disease. The Cobb angle decreased from 19.16±4.14 before CONTRAIS to 16.04±4.71 after CONTRAIS in the mild group (P<0.001). The Cobb angle decreased from 30.52±4.47 before CONTRAIS to 23.33±6.4 6after CONTRAIS in the moderate group (P<0.001). The Cobb angle decreased from 57.69±14.25 before CONTRAIS to 50.72±13.90 after CONTRAIS in the severe group (P<0.001). Based on these results, CONTRAIS was found to be effective for reducing total Cobb angles in the three symptom groups of AIS patients (Fig. 7).

CONTRAIS effects on total Cobb angles among the treatment groups. CONTRAIS, conservative treatment for adolescent idiopathic scoliosis. ***P<0.001.
CONTRAIS effects on thoracic spine Cobb angles among the treatment groups
The thoracic spine Cobb angle decreased from 18.85±4.33 before CONTRAIS to 14.59±4.62 after CONTRAIS in the mild group (P<0.001). The thoracic spine Cobb angle decreased from 20.98±5.90 before CONTRAIS to 15.47±6.63 6after CONTRAIS in the moderate group (P<0.001). The thoracic spine Cobb angle decreased from 31.87±8.87 before CONTRAIS to 28.05±8.27 after CONTRAIS in the severe group (P<0.001). Based on these results, CONTRAIS was found to be effective for reducing thoracic spine Cobb angles in the three symptom groups of AIS patients (Fig. 8).

CONTRAIS effects on thoracic spine Cobb angles among the treatment groups. CONTRAIS, conservative treatment for adolescent idiopathic scoliosis. ***P<0.001.
CONTRAIS effects on lumbar spine Cobb angles among the treatment groups
The lumbar spine Cobb angle decreased from 18.81±4.53 before CONTRAIS to 15.53±4.36 after CONTRAIS in the mild group (P<0.001). The lumbar spine Cobb angle decreased from 20.74±7.65 before CONTRAIS to 15.79±6.78 after CONTRAIS in the moderate group (P<0.001). The lumbar spine Cobb angle decreased from 30.08±7.77 before CONTRAIS to 26.41±7.57 after CONTRAIS in the severe group (P<0.001). Based on these results, CONTRAIS was found to be effective for reducing lumbar spine Cobb angles in the three symptom groups of AIS patients (Fig. 9).

CONTRAIS effects on lumbar spine Cobb angles among the treatment groups. CONTRAIS, conservative treatment for adolescent idiopathic scoliosis. ***P<0.001.
DISCUSSION
The positive result of CONTRAIS in the mild group was a reduction of 3.18°, 4.49°, and 3.28° in Cobb angles of the all, thoracic, and lumbar spine, respectively. The change in Cobb angle in the mild group was significantly reduced by CONTRAIS application. The positive result of CONTRAIS in the moderate group was a reduction of 7.19°, 5.51°, and 5.43° in Cobb angles of the all, thoracic, and lumbar spine, respectively. Cobb angle change in the moderate group decreased the most among the three groups by applying CONTRAIS. The positive result of CONTRAIS in the severe group was a reduction of 6.97°, 3.82°, and 3.67° in Cobb angles of the all, thoracic, and lumbar spine, respectively. Cobb angle change in the severe group was the second most significantly reduced among the three groups by applying CONTRAIS. These results demonstrate that CONTRAIS elicited effective outcomes for all AIS patients, regardless of their severity.
Although CONTRAIS is effective in the treatment of AIS, the general method for AIS in Korea is to check the Cobb angle by performing x-ray follow-up examinations every 6 months for AIS patients. This approach is no different than watching AIS get worse. In other words, without better treatment, x-ray follow-up is only followed, and eventually the Cobb angle progresses to more than 40° or the quality of life is seriously deteriorated due to cardiopulmonary insufficiency, which leads to surgery. Younger patients also develop adolescent depression or become less active in peer group activities. In this reality of AIS treatment, the introduction of CONTRAIS treatment is significant. In other words, if CONTRAIS is administered while AIS patients are waiting for follow-up every 6 months, patients with a Cobb angle of less than 10° can avoid scoliosis diagnosis, which will contribute to lowering the prevalence of AIS. In addition, it is expected to be able to deviate from the target of surgical treatment by improving the distorted appearance change in patients with a Cobb angle of 25° or more. CONTRAIS may help adolescents with scoliosis have a low quality of life and reduced self-esteem, and also when physicians consider more aggressive treatment (Dufvenberg et al., 2021). In the case of surgical treatment for AIS, there is a problem that postoperative pain is large in young patients, and most patients visit a hospital for pain treatment because the postoperative pain does not resolve (Kwan et al., 2020; Lee et al., 2020; Roye et al., 2022). Surgical treatment of the entire curved spine with pins can reduce spinal mobility in young patients and pose a risk of not reaching final growth, so this surgical treatment should not be considered a priority in the treatment of AIS.
In terms of the appropriate timing of scoliosis, this study can suggest that early detection and treatment through CONTRAIS enables successful correction of AIS as in previous studies (Anthony et al., 2021; Trobisch et al., 2010; Wong and Tan, 2010). Through this experiment, it was confirmed that CONTRAIS was effective in reducing Cobb angle in AIS patients. The effect of CONTRAIS on reducing Cobb angle did not differ according to the spinal region. Also, the Cobb angle reduction effect of CONTRAIS was more effective in severe cases.
ACKNOWLEDGMENTS
The author received no financial support for this article.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.