Effect of progressive resistance exercise using Thera-band on edema volume, upper limb function, and quality of life in patients with breast cancer-related lymphedema
Article information
Abstract
This study aimed to determine the effects of progressive resistive exercise (PRE), including complex decongestive physical therapy (CDPT), on edema volume, handgrip strength, upper extremity function, and quality of life (QoL) in patients with breast cancer-related lymphedema (BCRL). Twenty patients were randomized between the progressive resistance exercise group (PREG) and the self-home resistance exercise group (SREG). Two patients in each group dropped out of the study, leaving 16 patients: n=8 in the exercise group and n=8 in the SREG. First, the PREG and the SREG received CDPT. Subsequently, the patients in the PREG performed PRE, whereas the patients in the SREG performed self-home resistance exercises. Interventions were performed for 50 min, 3 times a week, for 6 weeks. The results showed that, for the edema volume, a significant intergroup variation was absent, whereas the intragroup variation was significant. The inter- and intragroup variations were significant for both handgrip strength and upper extremity function. Regarding QoL, a significant difference was observed in global health status/QoL and role function between the groups. Furthermore, significant differences were observed within the PREG in global health status/QoL; physical, role, and cognitive function; and dyspnea. No significant differences were observed within the SREG. The results collectively suggest that the exercise program was an intervention with a greater potential contribution to reducing edema and enhancing physical function in patients with BCRL.
INTRODUCTION
The most common treatment modality for breast cancer is surgery. If the tumor has spread to the lymph node, axillary lymph node dissection is likely to be performed (Theriault et al., 2013). Patients who undergo axillary lymph node dissection may experience breast cancer-related lymphedema (BCRL) as a complication (Harrington et al., 2011). Lymphedema is a chronic disease in which the protein component of lymph fluid stagnates in the interstitial space because of abnormal lymphatic circulation (Rebegea et al., 2015), causing loss of function, such as range of motion limitation, pain, atrophy, and stiffness of the affected upper limb (Cheema et al., 2008). These impairments negatively affect daily living and health-related quality of life (QoL) (Nesvold et al., 2010). The most common treatment modality for BCRL is complex decongestive physical therapy (CDPT) which combines comprehensive education on skin care, manual lymphatic drainage, and compression therapy (Haghighat et al., 2010; Huang et al., 2013).
As the survival rate of patients with BCRL improves, exercise intervention, another treatment modality, has been recognized as an important intervention method for improving physical function and lymphedema management (Cheema et al., 2008). In particular, upper extremity strength exercise helps the lymphatic circulation of the proximal part to effectively function the remaining lymph (Klassen et al., 2017). Among the intervention methods, progressive resistance exercise (PRE) of the upper extremity promotes the pumping function of venous and lymphatic fluid and contracts sympathetic nerves by improving muscular power and tension, leading to the alleviation of lymphedema (Kilbreath et al., 2012). Studies on low-to-moderate-intensity PRE of the upper extremity have reported that this intervention provides stability of upper extremity function and improves the QoL in patients with BCRL (Cormie et al., 2013). However, lymphedema can be aggravated if exercise intervention is performed incorrectly (Kilbreath et al., 2006). As a safeguard against this, most lymphedema treatments are performed together with CDPT (Klassen et al., 2017). Godoy et al. (2012) reported that the addition of compression therapy to PRE provide additional effects such as increasing lymphatic drainage through counterpressure generation and limiting vascular permeability because of changes in vascular pressure.
The Thera-band, which is widely used for strength training, has the advantage of applying to various classes because it provides resistance angles in various postures and has a low risk of injury (Lopes et al., 2019). However, there have been few studies on the application of Thera-band in patients with BCRL. Therefore, this study aimed to investigate the effects of CDPT and PRE on lymphedema and functional aspects of the upper extremities using a band in patients with BCRL.
MATERIALS AND METHODS
Patients
This study included 20 patients who received physical therapy from a rehabilitation specialist at the Catholic University of Korea Yeouido St. Mary’s Hospital in Seoul, South Korea, for the diagnosis of secondary upper limb BCRL after breast cancer surgery. The patients were randomized between the PRE group (PREG) and the self-home resistance exercise group (SREG). In each group, two patients dropped out from the study, leaving 16 patients: n=8 in the exercise group and n=8 in the SREG. The physical characteristics of the patients are shown in Table 1. This experiment was approved by the Research Ethics Committee of the Catholic University of Korea Yeouido St. Mary’s Hospital (IRB: SC19FESI0013). The experimental procedure is presented in Fig. 1.

Baseline characteristics of subjects
Consort flow diagram. PRED, progressive resistance exercise group; SREG, self-home resistance exercise group; K-DASH, Korean version of the disability of the arm, shoulder, and hand; EORTC, European Organization for Research and Treatment of Cancer; QLQ C30, core quality of life questionnaire 30.
Inclusion and exclusion criteria
The inclusion criteria in this study were individuals diagnosed with lymphedema after mastectomy, those who completed their courses of chemotherapy or had the plan to receive chemotherapy, those with current or completed radiotherapy after anti-cancer treatment, those who could perform exercise according to the therapist’s instructions, those who did not have a problem in cognitive functions, and those without abnormal findings on physical and neurological examinations. The exclusion criteria were current administration of chemotherapy, metastatic cancer, serious problems in the cardiopulmonary system, and orthopedic or neurological problems.
Study design
First, CDPT was applied to the PREG and the SREG. Subsequently, the patients in the PREG performed PRE using Thera-band, while the patients in the SREG performed self-home resistance exercises using Thera-band. The same investigator provided the rating before and after the intervention, and was applied for 50 min 3 times a week for 6 weeks.
Upper limb lymphedema circumference measurement
The arm circumference measurement method was used to measure the circumference of upper the extremity BCRL. Using a tape measure, the length between each marked point at 4-cm intervals from the ulnar styloid to the axillary on the affected upper limb was measured (12 parts in total), and the volume was calculated using the cone formula (Deltombe et al., 2007).
Grip strength measurement
A digital dynamometer (Model TKK 5401, La Fayette Instrument, Lafayette, LA, USA) was used to measure grip strength. Using the standardized method suggested by the American Society of Hand Therapists, the patients were instructed to pull the handle of the dynamometer with maximum strength in a sitting posture using the standardized method suggested by the American Society of Hand Therapists. The mean of triplicate measurements was estimated for both hands.
K-DASH measurement
The Korean version of the disability of the arm, shoulder, and hand (K-DASH) scale is a representative instrument used to assess hand, upper arm, and shoulder disabilities. It is a self-reported questionnaire developed by the American Academy of Orthopedic Surgeons. The scale consists of 30 base items and eight selections items. The basic items ask about the following issues: shoulder or hand problem (21 items); the severity of the pain, pain during activity, tingling, weakness, and stiffness (5 items); effects of disability on society, and degree of sleep; psychological effects (4 items). It consists of a 1-point to 5-point scale (1: no difficulty, 2: medium difficulty, 3: medium difficulty difficult, 4: very difficult, 5: not possible at all). The severity of disability increases as the score approaches 100, and the lack of disability is indicated by a score of zero. This study used only basic items due to the characteristics of the subjects (Wi et al., 2014).
Core QoL questionnaire 30 (QLQ C30) measurement
The European Organization for Research and Treatment of Cancer (EORTC) QLQ C30 (version 2.0) is a 30-item questionnaire for the evaluation of the health-related QoL of patients with cancer. It consists of multi-item and single-item scales and is mainly divided into global health status/QoL, functional, and symptom scales. All items are measured on a 4-point Likert scale, and two items out of global health status/QoL are measured on a 7-point scale (Demirci et al., 2011). All subscales met the reliability criteria (Cronbach alpha≥0.70) (Guzelant et al., 2004). EORTC QLQ C30 is shown in Fig. 2.

European Organization for Research and Treatment of Cancer (EORTC)-Core Quality of Life Questionnaire 30 (QLQ C30).
CDPT intervention
Both the PREG and SREG performed the following intervention thrice a week for 6 weeks: 15 min of MLD, 5 min of low elastic compression bandages, and 15 min of intermittent pneumatic compression therapy.
Progressive resistive exercise intervention
After the CDPT intervention thrice a week for 6 weeks, the patients in the PREG performed 50 min of PRE using a Thera-band. Warm-up and cool-down include breathing exercises and stretching. The main exercise was organized to stretch the thoracic muscle, stabilize the scapula, and strengthen the upper limb muscle in consideration of the subject’s shoulder joint disorder (Bok et al., 2016). Both arms were to perform 3 sets of 10 repetitions alternately. When the three colors of the Thera-band are stretched at 100% of the tissue length, the average tension is 15.7% yellow, 21.1% red, and 23.5% green (Thomas et al., 2005). The intensity of exercise was raised by changing the Thera-band color (resistance) one step every 2 weeks. Starting with yellow color in the first week, red color in the third week, and green color in the fifth week was applied. A 10-min warm-up and cool-down were performed before and after the exercise (Table 2).
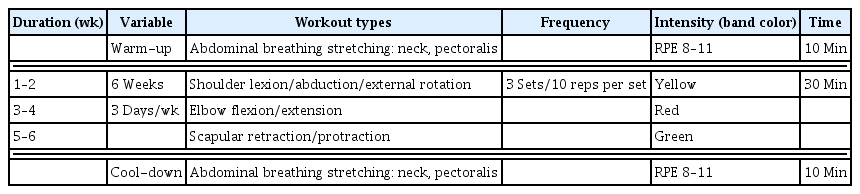
Progressive resistance exercise program using Thera-band
Self-home resistive exercise intervention
As with the PREG, the SREG received the CDPT intervention thrice a week for 6 weeks, and the patients in the SREG performed 50 min of self-home resistive exercise using a Thera-band. The warm-up and cool-down were the same as those of the PREG (Table 3).

Self-home resistive exercise program using Thera-band
Data analysis
Descriptive statistics and mean and standard deviation were obtained using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). Normal distribution was assessed using the Shapiro–Wilk test. To compare pre- and postexercise variations, the paired t-test and Wilcoxon signed-rank test were used. The independent t-test and Mann–Whitney test was used to compare the intergroup variations in the dependent variables. The significance level was set at P<0.05.
RESULTS
The results of the pre-homogeneity test for dependent variables (volume, grip strength, and K-DASH, EORTC QLQ C30 score) indicated homogeneity in both groups. Analysis of the changes in the dependent variable after the 6-week exercise intervention is as follows. Analysis of the changes in edema volume between groups showed no significance, but both groups within the groups showed significant differences (P<0.05). And after exercise intervention, the rate of change decreased by 5.41% in PREG and 4.47% in SREG (Table 4). Analysis of the changes in hand-grip strength showed significant between and within-group variations (P<0.05). And after exercise intervention, the rate of change increased by 32.58% in PREG and 4.46% in SREG (Table 5). Analysis of the changes in K-DASH showed significant between and within-group variations. And after exercise intervention, the rate of change decreased by 37.44% in PREG and 2.60% in SREG (Table 6). The QoL changes showed a significant difference between groups in the global health status/QoL and role function (P<0.05). Analyzing global health status/QoL, physical, role, cognitive, and dyspnea function within the group, the PREG showed significant differences (P<0.05), while there was no significant difference in the SREG. And the rate of change after exercise intervention increased by 47.17% in PREG and 6.77% in SREG in global health status/QoL, and physical function increased by 9.99% in PREG but decreased by 2.82% in SREG. Also, role function increased by 24.39% in PREG but decreased by 2.63% in SREG, and emotional function increased by 15.29% in PREG but decreased by 4.54% in SREG. In cognitive function, PREG increased by 11.36% and SREG by 4.26%, and in social function, PREG increased by 19.51% and SREG by 8.09%. In fatigue, PREG increased by 13.03% and SREG by 0.01%, and in nausea, PREG decreased by 31.98% and SREG by 10.49%. In pain, PREG decreased by 18.52% and SREG by 0.04%, and in dyspnea, PREG decreased by 33.33% and SREG by 0.02%. In appetite loss, PREG decreased by 23.07% and SREG by 0.02% and in constipation, PREG decreased by 23.07% and SREG by 15.38%. In diarrhea, PREG decreased by 25.01% and SREG by 19.99% and in Financial, PREG decreased by 0.03% and SREG increased by 18.17% (Table 7).

Changes in the edema volume
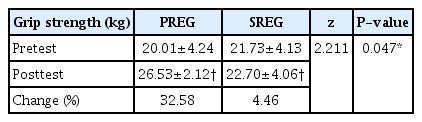
Changes in the grip strength
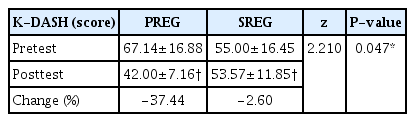
Changes in the K-DASH

Changes in the EORTC QLQ-C30
DISCUSSION
This study investigated the changes in edema volume, grip strength, and upper extremity function after the application of CDPT and PRE using Thera-band for 6 weeks for therapeutic management in patients with BCRL. The results showed that there were significant within-group differences (P<0.05), but no significant between-group differences in the edema volume of the upper limb. In particular, the rate of decrease was higher in the PREG than in the SREG (−5.41% vs. −4.47%). Patients with BCRL have an abnormal accumulation of tissue fluid due to impaired lymphatic circulation, and when this condition persists, protein-rich fluid accumulates and causes swelling of the affected subcutaneous tissue (Korpan et al., 2011). Therefore, the exercise intervention in this study helped to reduce the amount of edema by promoting the movement of abnormally accumulated lymph fluid to the lymph nodes by increasing protein reabsorption into lymphatic vessels through strengthening muscle strength and contractility (Franzeck et al., 1997). Kilbreath et al. (2006) reported that pain and swelling decreased 4 weeks after starting exercise as a result of applying PRE and stretching for 8 weeks to BCRL patients aged 40–65 years, which is consistent with the results of this study. In this study, the edema volume decreased more in the PREG than in the SREG, suggesting that PRE is more effective than self-home resistance exercise in patients with BCRL.
Patients with BCRL complain of many aspects of ADL (Baumann et al., 2018) owing to decreased muscle strength and physical ability, such as hand grip and upper limb dysfunction, caused by edema (Smoot et al., 2010). Accordingly, this study investigated the changes in hand grip and upper limb strength after 6 weeks of intervention and found that there were significant between-group and within-group differences (P<0.05). After the intervention, grip strength improved by 32.58% in the PREG and by 4.46% in the SREG. The K-DASH score also decreased by 37.44% in the PREG and 2.60% in the SREG, after the intervention. These results suggest that the intervention applied to the PREG is more effective than Ammitzbøll et al. (2019). Applied PRE as a group exercise for 20 weeks and self-exercise for 30 weeks in patients with BCRL and reported a decrease in edema volume and significant improvement in body function. Bok et al. (2016) reported that the application of PRE and CDPT for 8 weeks increased the muscle thickness of the upper extremity in patients with BCRL. As a decrease in edema volume has been shown to improve muscle and joint movement and increase lymphatic flow (Ammitzbøll et al., 2019), the results of this study showed that it contributed to the improvement of hand grip and upper limb function. Ergun et al. (2013) reported that a gradual increase in exercise intensity rather than low-intensity exercise helps to reduce swelling and improve muscle strength and range of motion. These previous studies mean that gradual resistance exercise is more effective in increasing muscle strength and improving function than low-intensity exercise.
Since the patients performing Thera-band exercise should maintain grip strength to hold the band with both hands, an increase in exercise intensity leads to an increase in grip strength. Blood flow in the forearm, which increases with an increase in grip force, reaches a maximum at 30% of the maximum contractile grip force (Stanton et al., 2009), and the increase in capillary permeability in this process leads to increased lymphatic production (Sakakibara et al., 1990).
Lymphedema and limitations in upper extremity function in patients with BCRL lead to difficulties in daily life, resulting in decreased QoL (Rietman et al., 2003). In this study, EORTC QLQ C30 showed a significant difference between the groups in terms of global health status/QoL and role function (P<0.05). Within the group, the PREG showed significant differences in global health status/QoL; physical, role, and cognitive functions, and dyspnea (P<0.05), indicating an improvement in QoL. However, there was no significant difference in symptom scales other than insomnia. This is because BCRL is associated with radiotherapy and cancer treatment (Borman et al., 2021). In contrast, no significant difference was noted in the SREG for any items (Table 6). Most of the variables on the symptoms scale did not show significant differences because they were related to the subjects’ radiation therapy and cancer treatment.
Ahmed et al. (2008) reported that upper extremity problems due to lymphedema affect daily activities and social life and increase psychological stress. Therefore, in the results of this study, it is judged that the significant difference in many variables of the scale of the function was due to the improvement of upper extremity function problems. Kilbreath et al. (2012) reported an improvement in lymphedema and upper extremity function after PRE, indicating that it is a direct factor that improves the QoL. Do et al. (2015) reported that the QoL of patients with BCRL improved according to the EORTC QLQ C30 evaluation after performing a combination of CDPT and resistance exercises, showing their correlation with lymphedema reduction and improvement of functional disability. Borman et al. (2021) reported that, according to the EORTC QLQ C30 evaluation, QoL had improved in patients with BCRL who had reduced lymphedema through treatment intervention, and a high QoL improvement can be expected the sooner the intervention. These results support the idea that Thera-band exercise in this study contributed to the reduction in edema volume as well as the improvement of grip strength, upper limb function, and QoL. Although the effectiveness of resistance exercise in patients with BCRL has been continuously reported, it should be noted that the resistance exercise may aggravate lymphedema (Kilbreath et al., 2006). This study investigated the effectiveness of CDPT and PRE using Thera-band in patients with BCRL. It was found that PRE is more effective than self-home resistance exercise in decreasing edema volume, improving upper function ability, QoL and the accompaniment of CDPT to exercise is a safer treatment option for lymphedema. Future studies on PRE in patients with BCRL are recommended to consider various factors, such as psychological factors, complications, and recovery speed. However, our study has limitations such as the small number of subjects and short duration, making it difficult to generalize to all patients with upper extremity lymphedema. In future studies, exercise programs should be conducted with more subjects from a long-term perspective.
ACKNOWLEDGMENTS
The work was supported by the research fund supported by the College of Culture and Sports at Korea University in 2022.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.