INTRODUCTION
Persons with physical disabilities (PPDs) face challenges with regard to maintaining physical fitness due to inactivity and concomitant medical factors. PPDs trend towards less physical activity than those without physical impairments (Glattke et al., 2022), and have been shown to exhibit a reduced quality of life (QoL) and restricted community integration. Moreover, physical inactivity and a lack of physical fitness can exacerbate functional limitations (Garber, 2019). The American College of Sports Medicine categorizes health-related physical fitness components into a five-component grouping consisting of cardiorespiratory endurance, muscular strength, muscular endurance, body composition, and flexibility (Jeong et al., 2020). In the interest of maximizing these parameters to improve QoL in PPDs, there is an increasing emphasis on sport participation for these individuals. In this regard, “adapted/adaptive sports,” or activities that have been modified to allow access for PPDs, have expanded significantly in popularity in recent years (Grams et al., 2016).
Wheelchair basketball (WB) was created in 1946 as a means of rehabilitation for an injured World War II serviceman in the United States. On September 25, 1946, a group of combat veterans in the United States played the first official WB game. A league-level game was first played at the International Stoke Mandeville Games in 1956. From this origin, WB grew quickly. In response to widespread acceptance of the sport globally, the International Stoke Mandeville Games Federation was established in 1973 as the first WB federation. In 1989, the name was changed to the International Wheelchair Basketball Federation (IWBF). Since 1975, the Federation has staged official world championships held biannually after the summer Paralympic Games (Glattke et al., 2022). WB has been a paralympic sport since the inaugural Paralympic Games in Rome in 1960, and it is now played in over 100 nations (Glattke et al., 2022).
Given fundamental differences in player movement, the types of errors that are made, and the functional classification of individuals on the court, WB game regulations differ from traditional basketball game rules. Despite this, WB is played with in-game rules that are nearly comparable to the International Basketball Federation (FIBA) rules. Games last 40 minutes, and court and ball size, half-court rules, duration of shot clocks, personal foul counts and regulations, height of baskets, and point scoring systems are all congruous with FIBA rules. The key difference between traditional basketball and WB, is the classification system which governs WB.
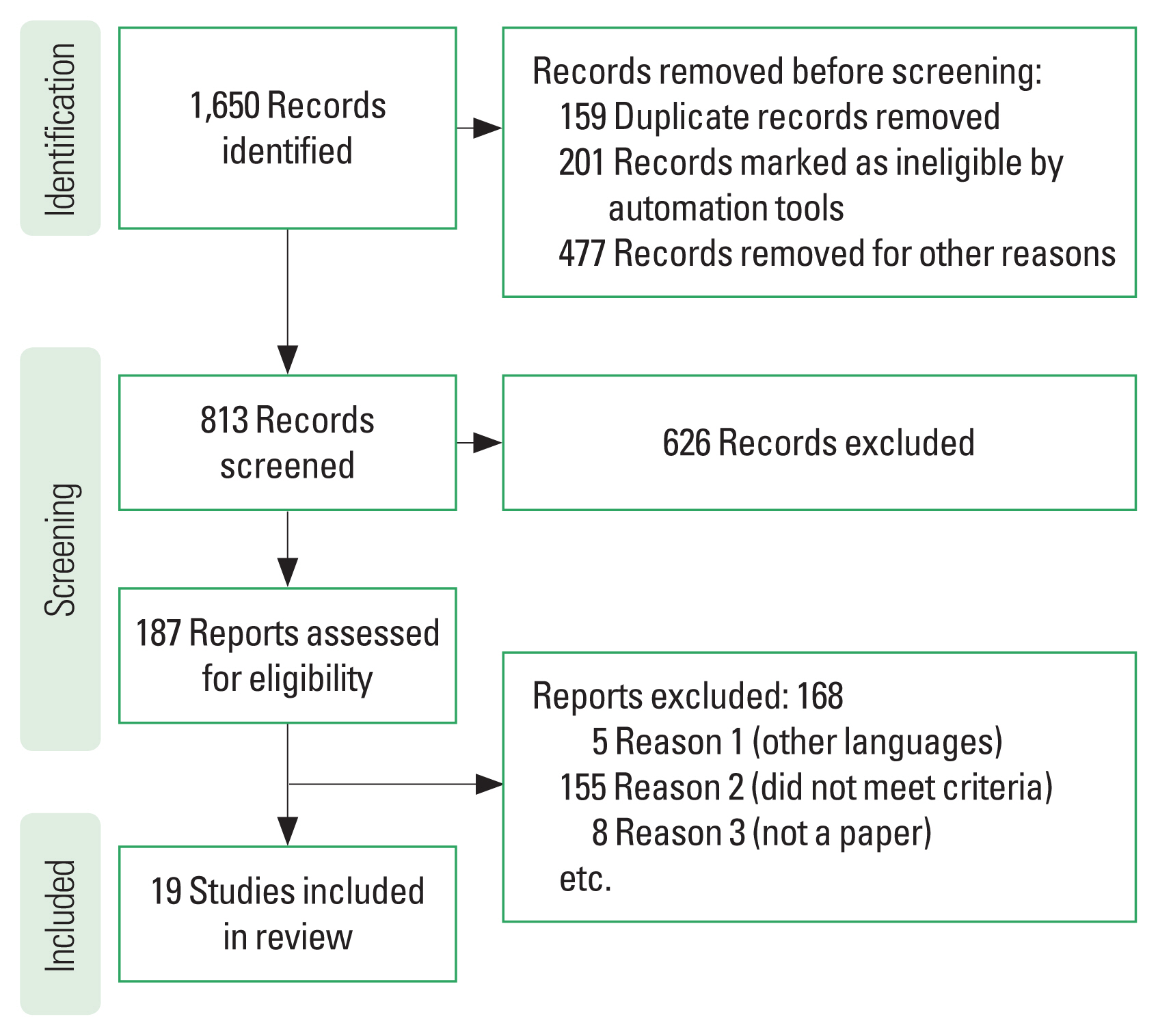
A variety of durable benefits resulting from participation in adapted sports is reported by a recent study (Molik et al., 2017). In the physical domain, PPDs experience substantial benefits with regard to improved functionality (Grams et al., 2016) and demonstrate greater rates of ventilatory threshold, maximal oxygen uptake, and other markers of aerobic fitness (Molik et al., 2017). One such adapted sport is WB. Athletes with physical restrictions such as those with spinal cord injury, post-poliomyelitis sequelae, amputations, cerebral palsy, and other conditions can participate in WB (Crespo-Ruiz and Del Ama-Espinosa, 2011). Given the rise in popularity of WB in recent years both due to its enjoyability for participants and as a spectator (Fliess Douer et al., 2021; Molik et al., 2017), a literature review is indicated focused on both the health aspects of participation in the sport as well as areas of emphasis for competitive advantage for athletes looking to maximize their performance (Rice et al., 2016). Fig. 1 shows the identification and inclusion flowchart for the analyzed studies. Therefore, the purpose of this study was to review the various risks and benefits of WB and explore some of the research which outlines factors that influence WB player performance and conditioning.
HEALTH BENEFITS OF WHEELCHAIR BASKETBALL
Physical benefits
Regular exercise is beneficial for PPDs and the non-physically disabled. PPDs who participate in a variety of exercises have been shown to demonstrate enhanced blood circulation parameters, improved cardiac and pulmonary function, increased maximum stroke volume or cardiac output, and lower chances of hip or vertebral fracture. Moreover, regular exercise may improve blood cholesterol levels, enhance weight control and everyday activity capacity, increase muscular strength, and help reduce the risk of the development of a number of chronic illnesses (García-Gómez et al., 2019). In this regard, it appears that WB serves as an excellent form of exercise.
Several studies have attempted to measure WB’s influence on physical fitness. One of the recent researches evaluated the aerobic and anaerobic performance of 17 highly trained WB athletes to see if there was a relationship between the IWBF functional categorization system and cardiorespiratory endurance. Participants in that study completed cardiopulmonary exercise testing and a Wingate-like 30-sec sprint test to determine power output. The findings revealed a link between the IWBF functional categorization scheme and the outcomes. Power output, as well as anaerobic and aerobic performance rose with functional categorization. Similarly, the other study found that WB players have higher aerobic fitness levels than their non-exercising peers (Molik et al., 2017). Also, a previous study demonstrated significant power output disparities between WB players and inactive people with physical limitations (García-Gómez et al., 2019). Likewise, cardiorespiratory endurance may be a significant predictor of competition level in WB with peak oxygen consumption correlating with increased competitive status of WB players (Mueller et al., 2021). Furthermore, WB can beneficially impact cardiac risk profile. According to a study that investigated the effect of WB on the lipid profile of female paraplegic patients and concluded that weekly WB activity improved lipid profile test results in paraplegic patients and may lower cardiovascular risk factors (Kargarfard et al., 2018).
In addition to improving metrics of cardiorespiratory and metabolic fitness, WB has the potential to greatly improve muscular strength. Significant upper extremity muscular strength is required to perform the complex and taxing operations necessary to participate in the sport. When the wheelchair is in active use for more than 10–20 min, shoulder muscular activation occurs at high levels, causing selective muscular hypertrophy. WB players have high levels of concentric-eccentric power in their shoulder rotator cuff muscles (Campos et al., 2021). Furthermore, data suggest that WB players had greater rotator cuff muscular strength than non-athlete populations with paraplegia. Taken one step further, WB players may have even stronger shoulder flexor and extensor muscles than nondisabled persons (Tsunoda et al., 2021). Unfortunately, no study to our knowledge has directly compared physical benefits conferred from WB to other sports such as swimming.
Psychological benefits
PPDs may experience restricted community inclusion and subsequent adverse effects on mental health compared to those without disabilities (Grams et al., 2016). Thus, adapted sports may have benefits beyond the documented improvements in physical health. Participants in adapted sports express feelings of empowerment decreased anxiety and depressive-type symptomology, and often experience significant motivation to continue participating in the sport (Lim et al., 2017). Studies have shown improved QoL, general health, and life satisfaction scores in adapted sports athletes (Grams et al., 2016). Likewise, other studies showed that involvement in community-based therapeutic leisure and adaptive sports programs can improve not only general health, but family- and social-life quality (Groff et al., 2009). These findings extend to sports activity with a rehabilitation focus as well (Fiorilli et al., 2013). Research has also indicated improvements in feelings of empowerment, self-efficacy beliefs, and enthusiasm for continuing engagement in the sport activity. It was also demonstrated stronger peer relationships and higher social connections than those who do not participate in adaptive sports (Giacobbi et al., 2008). Adaptive sports can lead to a more positive self-image and can enhance participation in significant life activities and responsibilities outside of sports (Molik et al., 2017).
The psychological benefits of adapted sports have been shown to extend to WB as well. Fiorilli et al. (2013) determined that WB athletes had higher psychological health than those with lower limb impairments who did not participate in sports. Moreover, long-term WB athletes had greater psychological health than short-term athletes, suggesting a dose-dependent response of WB. This finding was corroborated by another study that compared the mood states of 26 WB athletes to the mood states of 28 PPDs who used wheelchairs but did not engage in any activity and found that WB athletes had much lower levels of depression than non-athletes and that wheelchair sports played a critical role in the well-being of the athletes, providing several advantages (Paulsen et al., 1990). Taken in summation, WB is a powerful tool for psychological benefit in PPDs.
MOTIVATIONAL FACTORS
To thrive in sports, athletes must be personally, or intrinsically, motivated to participate and excel at the chosen sport (Mudrak et al., 2018). Adapted sports can bring significant advantages to participants. However, these benefits will not be realized if the athlete is not consistently engaged. Athletes who are motivated by external factors such as monetary gain may lack autonomy and feelings of competence, which ultimately may lead to decreased interest in the sport. Previous research has demonstrated that there is no variation in motivation between low-point and high-point players and determined that players are mostly task-oriented (Fliess Douer et al., 2021). That finding implies that physical limitation in WB athletes does not influence goal perspective. Another study questioned 10 female WB players aged 18 to 32 years about their experiences competing at the highest level (Ashton-Shaeffer et al., 2001) and semistructured interviews revealed two major themes. The first subject dealt with resistance and the use of sport to combat stereotypes of disability, sport, and femininity. The second subject dealt with empowerment as a result of sports experiences. Despite the participants being exceptional high-level athletes, they identified the origins of their interest in the sport as being related to the community aspects of WB.
Other research has compared WB athletes and able-bodied basketball players with regards to sport accomplishment orientation (Skordilis et al., 2002). Findings demonstrate that WB athletes scored better on goal orientation and competitiveness ratings than able-bodied basketball players. This research implies that WB players participate in basketball to achieve personal objectives and compete against their peers more so than their able-bodied counterparts (Skordilis et al., 2002). Despite this finding, the data demonstrated that the game outcome was unimportant to either group. Research has also compared the motivational factors of 57 WB players to those of 70 nondisabled basketball players (Dehghansai et al., 2021). That study assessed task and ego orientation, self-efficacy, and items related to family encouragement and athletic participation. Their findings revealed no change in self-efficacy across the groups. Nonetheless, non-PPD athletes outperformed their WB counterparts in both task and ego orientation. WB athletes, on the other hand, scored higher with regards to familial support. Finally, low-point WB players were shown to have worse self-efficacy than high-point players (Dehghansai et al., 2021). The study investigated the coping abilities and motivation of nondisabled and WB basketball players and found contradictory results (Dehghansai et al., 2021). While female WB players scored higher on intrinsic motivation than male WB players, they rated worse on introjection. However, both able-bodied and disabled athletes performed similarly in terms of coping abilities. Thus, these authors found that the two groups had similar motivation for playing basketball and had similar coping skills and methodologies.
WHEELCHAIR BASKETBALL AS A COMPETITIVE SPORT
Classification schema
The international WB classification system allows for the participation of PPDs with a wide variety of functional abilities while promoting high levels of competition and performance. Emphasis is placed on ensuring equal balance in functional ability between competing teams (Molik et al., 2017), and WB classification schema has evolved over time to address that need more adequately. Only PPDs with spinal cord injury or amputation competed during the early post-World War II period, and a medical diagnostic was used to place the athletes in one of three groups. As more individuals with disabilities became interested in the game, the classification allocation algorithm was found to be deficient and was modified. One study developed a WB-specific functional categorization system in 1978, and this system was formally approved in 1982 (Molik et al., 2017).
Strohkendl’s method is “based on a player’s physical ability to perform essential basketball actions such as moving the wheelchair, dribbling, shooting, passing and catching, rebounding, and responding to contact.” According to the 2014 WB classification guideline, a player’s classification is determined by three key items: (1) trunk control, (2) lower extremity contribution, and (3) upper extremity functional limitation (Glattke et al., 2022). The first and most important item refers to trunk control or lack thereof. The IWBF classification manual defines trunk control as the amount to which a player may move freely in any direction and return to the upright sitting position without gripping the wheelchair for support or utilizing the upper limbs to aid in the movement. This concept encompasses all directions and depicts the ball’s location as if the player were holding it with both hands (Glattke et al., 2022). The study investigated trunk motions in reference to WB classification schema and concluded that the present WB categorization method adequately classifies players based on functional capacity to compete in WB (Haycraft et al., 2022). The second item in the classification guideline refers to function of the lower extremities. Use of the lower extremities to aid in pelvic control and general stability is assessed. The third and final item evaluates upper extremity function and ability to perform wheelchair movement and ball-handling skills such as passing, dribbling, and shooting.
Based on the IWBF three-item functional level classification schema, eight different classes are defined: 1.0, 1.5, 2.0, 2.5, 3.0, 3.5, 4.0, and 4.5. These classes each have their own functional profile and detailed characterization of the expected volume and level of activity. When players fall between two classes, one of the borderline categorizations (i.e., 1.5, 2.5, or 3.5) is considered. The 4.5 class identifies a player with the least significant influence of their respective disability on WB performance (Glattke et al., 2022). According to current IWBF rules, the total point restriction for a team’s five players at any given moment is 14 points (e.g., 1 pt+ 2 pt+3 pt+3.5 pt+4.5 pt=14 pt) (Glattke et al., 2022). To further increase inclusivity of the sport, the IWBF has advocated for admission of female and junior athletes to male national league competition. To accomplish this while still creating fair team balance, when a female or junior athlete competes in Euroleague events, for example, the permissible total team points may increase by 1.5 points.
With the introduction of this complex eight class system to maximize inclusivity of the sport while maintaining competitive level, WB was the first adapted sport to use a functional classification schema rather than a medical categorization system. Other paralympic classification systems have followed suit, with the intention of reducing the influence of eligible forms of disability on team disparities to create a level playing field for all athletes to maximize enjoyment of the game and feelings of “fair play” (Fliess Douer et al., 2021).
Competitive advantage in WB
While maximal inclusivity is a goal of WB, this does not detract from the intensely competitive nature of the game. WB athletes strive to excel at their craft, and train at extremely high levels to maximize their performance. Given the unique demands of the sport, much research has explored various training, lifestyle, and rehabilitative techniques to optimize WB sport performance while reducing injury risk. Previous research has outlined several beneficial effects of WB-tailored workouts in strengthening the abilities of wheelchair sprinting and shooting for WB players (Cools et al., 2021). The impact of kinesiotaping on WB player’s shoulder muscular strength has also been studied, with the results indicating that tape application may boost isokinetic muscle strength (Reynard et al., 2018). In researching less commonly applied performance-improvement tactics, it was found that mindfulness training increased athlete’s health and performance (Anderson et al., 2021). That study found improved focus and awareness levels, stress management ability, sleep quality, heart rate (HR) variability control, and foul shot accuracy after this intervention was applied.
Proper cardiorespiratory conditioning is also critical to optimal performance in WB. It was concluded that respiratory muscle strength may improve WB player’s aerobic threshold, and thereby improve in-game cardiorespiratory endurance (Sanz-Santiago et al., 2020). The other study determined that that the aerobic performance of WB players varies with playing experience, age, and handicap (Bayrakdaroglu et al., 2022). According to that study, the 35- to 45-year age group demonstrates the lowest cardiorespiratory endurance performance levels. Additionally, it was found that severity of impairment has the most significant impact on the aerobic performance of lower functional level (i.e., 1–1.5 point) WB players. Long-term WB athletes who had participated for six to 10 years had the best cardiorespiratory endurance performance values (Bayrakdaroglu et al., 2022).
WHEELCHAIR BIOMECHANICS, KINEMATICS, AND ERGONOMICS
Wheelchair mobility in performing quick-turning, forward, and reverse patterns is paramount to optimal performance in WB (De Freitas et al., 2023). While proper muscular and aerobic training is critical to ensure optimal gameplay, ergonomic factors of the wheelchair can impact mobility significantly and should be carefully tailored to each athlete. Wheelchair type and build should also take impairment level into account (Veeger et al., 2019). The frame, front wheels, backrest, footrest, antitip mechanism, rear axle, and main wheels are the essential components of a WB wheelchair (De Freitas et al., 2023).
The effect of wheelchair mass is a topic of current investigation. Present research indicates that additional mass (5- and 10-kg increments) do not significantly increase physical strain in a study with non-PPD participants on a wheelchair treadmill (Cowan et al., 2009). The study investigated these results and found no effect of added bulk (5 kg) on sprint performance, but did note a drop in performance in the Stop-and-Go test (Sagawa et al., 2010). In contradiction, one study found that increasing the mass of the wheelchair by 9.05 kg reduced mean self-selected velocity (Cowan et al., 2009). Some research has suggested that WB injury profile may be influenced by wheelchair design. Higher-quality, lighter-weight competition wheelchairs with frictionless bearings may boost mechanical efficiency and reduce injury burden. Thus, mass reduction is a goal in most modern-design WB wheelchairs. However, wheelchair cost may become prohibitive. Thus, heavy, earlier-model wheelchairs are commonly utilized in lower-level league play (Tachibana et al., 2019).
Alternative wheelchair and interface configurations can be considered based on WB functional level categorization (De Freitas et al., 2023). Active trunk stability and rotation have been identified as essential performance variables and are critical factors in the current WB categorization scheme (Rice et al., 2022). Lower-category players, therefore, may be unable to adjust for the greater distance between the wheelchair handrail and their shoulder center of rotation when in higher seat positions. Furthermore, players with lower classifications generally have lower power outputs than those with higher classifications, further exacerbating this discrepancy (Gil et al., 2015). In response to these concerns, in a systematic field-based examination of elite WB players, a researcher investigated the influence of seat height, mass, and glove wear on mobility performance (Rietveld et al., 2021). That study determined that (1) lowering the seat height by 7.5% resulted in faster performance on wheelchair mobility performance testing, and (2) adding 7.5% more mass to the wheelchair and the use of gloves did not result in a significant difference in performance. These findings held true regardless of categorization, with both high- and low-classification players responding similarly to the interventions.
COMMON WHEELCHAIR BASKETBALL INJURIES, AND THEIR PREVENTION AND TREATMENT
Intensive training sessions and high-level tournament play raise the risk of trauma and sports-related injuries. Injury pathophysiology in wheelchair athletes is multifactorial. Overuse injuries account for 23%–52% of all injuries soft tissue injuries, and injuries particularly to the upper extremity are common in wheelchair athletics (Fagher et al.,2020). According to Curtis and Dillon (1985), 72% of wheelchair athletes have suffered at least one injury from their sport activity. WB may be particularly high risk, accounting for 24% of all injuries reported in the study. An epidemiological survey of sport-related injuries in WB reveals 54% of athletes reporting significant discomfort during sport, with upper extremity pain accounting for 79% of the overall incidence (Yengo-Kahn et al., 2021). Another study has described high rates of finger injuries from wheelchair collisions and a high incidence of concussion in WB (Wessels et al., 2012). Given the high rates of injury in the sport, education on injury prevention is encouraged, a thorough warm-up is recommended, and hand protection is imperative. It is important to note that specific injuries may require additional rehabilitative efforts, and coaches, athletes, and trainers alike should be attuned to recognition and treatment of these injuries.
Specific upper extremity injuries in WB
Many studies have reported an increase in musculoskeletal injuries among wheelchair athletes. The most commonly reported acute injuries are strains of the metacarpophalangeal joints, while tendonitis or tendinopathy of the shoulder is the most commonly characterized repetitive strain injury. Injury is a major cause of loss of time on the court: 52% of patients miss no more than seven days of training after an injury, 29% miss between 8 and 21 days, and 19% miss more than 22 days. The demands of wheelchair propulsion and the weight-bearing necessary for transfers and everyday activities place undue strain on the upper limbs. This is because the upper limb is designed for movement rather than stability, which may predispose individuals to injury (Yengo-Kahn et al., 2021).
Problematically, WB players are at a heightened risk of upper extremity overuse injuries, particularly of the shoulder, due to frequent usage for wheelchair propulsion. While wheelchair propulsion itself is demanding (Heyward et al., 2017), sports involving overhead throwing, such as basketball, apply additional stress to the shoulder (Tsunoda et al., 2021). Thus, experiencing some degree of shoulder discomfort among WB players is almost ubiquitous to the sport (Yıldırım et al., 2019). One study reported a 50.7% prevalence of sports-related muscular discomfort among athletes with locomotor impairments, with the most common affected area being the shoulder. Of these athletes, 58.8% were WB players (Bernardi et al., 2003). A variety of additional factors have been identified to further exacerbate shoulder and upper extremity issues in WB athletes (Yıldırım et al., 2019). The seated posture of WB athletes, particularly those with spinal cord injuries, includes a posterior pelvic tilt, a forward head position, and greater thoracic kyphosis. This posture causes the shoulder girdle to be shifted anteriorly, putting additional pressure on the neck and upper back, and decreasing scapula-thoracic function. Further, inadequate strengthening regimens for the scapula and rotator cuff muscles may result in muscular imbalances in these athletes (Yıldırım et al., 2019).
Specifically, impingement syndrome is thought to be one of the most common causes of shoulder discomfort and/or injury in wheelchair athletes, with several contributing factors (Heyward et al., 2017). For example, inadequate recovery periods due to the wheelchair athlete’s desire to continue to participate in sports may contribute to overuse. At more competitive levels, due to intense training regimens and participation in several athletic competitions and league tournaments throughout the year, wheelchair athletes have limited opportunities to relax and recover. Furthermore, because the wheelchair-bound athlete is closer to the ground than an able-bodied athlete, motions such as flexion and abduction of the shoulder are made continually in daily tasks such as reaching up for an object, as well as for WB activities such as shooting, rebounding, and passing. Scapular protraction and internal rotation of the shoulder have also been reported with vigorous propulsion during wheelchair use (Heyward et al., 2017).
With regard to ameliorative options for shoulder pain, WB athletes may require frequent evaluations and a coordinated, multidisciplinary team approach with extensive input from clubs and institutions to develop and implement appropriate regimens. An interventional study found that a shoulder home-based workout program was a good aid for preserving WB players’ shoulder conditions throughout their training regimes when preparing for top WB tournaments such as the Paralympic Games (García-Gómez et al., 2019). Further work is needed to establish the efficiency of other shoulder home-based workout programs in larger sample sizes, and to integrate and investigate preventative programs in the training of younger players (García-Gómez et al., 2019). Moreover, a simple and reliable evaluation method for monitoring the shoulder condition of wheelchair athletes is required (Tsunoda et al., 2021).
Although the shoulder appears to be the most common site of injury and/or pain in wheelchair athletes, one study found that the cervical (59%) and thoracic spine (8%) were the primary sites of referred pain to the shoulder in a study of British athletes competing in the Paralympic Games (Heyward et al., 2017). Likewise, trunk control is thought to contribute to upper extremity symptoms. Despite this, the study reported that 62% of players with trunk control and 56% without trunk control suffered some elbow and/or wrist pain during wheelchair use (Yıldırım et al., 2019). However, more research is needed to define the contribution of trunk control to shoulder and elbow pain.
Distal to the shoulder, carpal tunnel syndrome (CTS) is the most prevalent condition affecting wheelchair athletes (Asheghan et al., 2016). The thumb, index, middle, and lateral parts of the fourth finger are affected, as is the abductor policies Brevis muscle. Aching discomfort in these areas of the hand is a common finding in WB athletes (Heyward et al., 2017), and CTS has a reported prevalence of 52%–100% of wheelchair users electro-diagnostically. Despite this finding, CTS is only present in 7%–67% of athletes clinically, and the use of padded gloves to relieve pressure on the carpal tunnel and prevent blisters and sores is recommended (Rice et al., 2022). Soft tissue injury, such as to the pronator teres muscle and the remainder of the wrist flexors, has been observed to occur during the acceleration phase of throwing in WB, leading to medial epicondylitis. Other lower extremity issues affecting WB athletes include ulnar neuropathy and carpal instability due to repetitive microtrauma to the wrist (Asheghan et al., 2016).
Specific lower extremity injuries in WB
While the upper extremity is more commonly affected in WB, several injuries can occur to the lower extremities as well. Tendon and ligament injuries in the contralateral and residual limbs as well as broken skin from prosthesis rubbing at the distal end of the residual limb are common in athletes with amputations. Amputees have a high prevalence of pain with sport (75%), and it has been proposed that sport-specific prostheses may increase an athlete’s performance and reduce pain by decreasing compensation of the residual limb (Grobler and Derman, 2018). Additionally, spinal cord injury may decrease bone density below the injury level due to limited weight bearing, resulting in osteopenia or osteoporosis and an increased risk of fractures (Morse et al., 2019). It has been reported that WB has the highest risk for fractures due to direct contact and falls when compared to other wheelchair sports (Patatoukas et al., 2011), and athletes with spinal cord injuries are more susceptible to fractures (Morse et al., 2019).
PHYSIOLOGICAL DEMANDS OF WHEELCHAIR BASKETBALL
WB induces high cardiovascular demand. Athletes display a HR equivalent to values over the anaerobic threshold for about 68% of playtime and a majority of the game may be spent above the lactate turn-point for many athletes (Croft et al., 2010). While research reports a lower percent time above the anaerobic threshold (28% of the playtime), WB remains a high-intensity exercise (Seron et al., 2019). In absolute terms, the HR mean values for players varied between 148 and 163 beats per min (beats/min) during a game of WB. HR peaks were found to be 174 beats/min when assessing only two-quarters of the game and 190 beats/min when monitoring throughout the game (Croft et al., 2010). Another study evaluated HR before and after games in 20 WB top players (10 with neurological disorders and 10 with musculoskeletal problems) during the International WB Championship in Edmonton, Canada and found that athletes with SCI had smaller increases in HR one hour after beginning gameplay than athletes with musculoskeletal impairments (Heyward et al., 2017). Moreover, although elevated HR may induce temperature increases that can raise the risk of hyperthermia, no incidence of heat-related illness occurred in WB athletes during gameplay analysis. Regardless, WB appears to have significant cardiovascular demands with elevated HR throughout gameplay, necessitating high-intensity training to prepare for the physiological requirements of the game (Seron et al., 2019).
WHEELCHAIR BASKETBALL MATCH ANALYSIS
WB has become one of the most popular paralympic sports. A complex set of skills are required for shooting a ball from distance, completing layup shots, transferring the ball between players, doing overhead passes, dribbling, and engaging in other play-related activities (Cavedon et al., 2015). WB match-play is characterized by high-intensity intermittent efforts in which accelerative wheeling sprint capacity from a standstill and over short distances play a significant role in in-game performance. Thus, physical strength and power output are paramount to success in WB (Ferro et al., 2016). Croft et al. (2010) have emphasized training at high intensity for shooting, dynamic movement, and rebounding activities for optimal game-ready performance. That study demonstrated improvements in WB players who practice more half-court games to expeditiously train high-intensity technical skills such as turnovers, rotations, rebounding, and shooting (Mason et al., 2018).
While high-intensity training is critical to success in WB, more technical, skill-based training is also fundamental to in-game development. WB players continuously work to enhance their wheelchair movement skills. WB major maneuver operations are divided into two categories: “push” and “pull.” “Push” refers to gripping the rim and pushing it forward to accelerate the wheel, while “pull” refers to grabbing the rim and halting forward progression of the wheels to decelerate the wheelchair. In other words, the “push” action applies force to the wheel in the forward direction, while the “pull” motion applies force in the opposite (backward) direction (Jansen et al., 2002). Additionally, the pivot turn is one of the most crucial tactics to master in WB, as its use allows for a player to effectively push an opponent away to create distance for a shot or pass maneuver. During match analysis of a WB practice game, a total of 1,005 “push” and 152 “pull” actions, 172 pivots, and 192 turn actions were recorded. In WB, it can be difficult to abruptly shift the travelling direction of the wheel. Thus, some players rely on their dominant hands and make consecutive turns in the same direction. Furthermore, complex movements are necessary to evade or interfere with opponents, so multiple maneuver types are often artfully combined (Jansen et al., 2002).
Research has previously described effective strategies for WB play through match analysis and reported a variety of types of activities during gameplay. Players spent 8.9% of their time actively moving the wheelchair at fast pace, 23.5% gliding, 18.2% wrestling for the ball, 0.6% sprinting with the ball, 0.3% shooting, and the remaining 48.3% remaining motionless or on the bench (Johansson et al., 2015). It was also revealed that during game conditions, the length of concerted efforts varies from less than 20 sec in 47.1% of the instances to more than 60 seconds in 11.8% of the cases (Giancamilli et al., 2022). In summation, match analysis of WB demonstrates substantial work outputs required during gameplay and a wide variety of different movements and skills employed throughout the match.
WHEELCHAIR BASKETBALL AND SLEEP
Sleep has been recognized as a significant factor influencing sports performance across a wide array of athletic endeavors (Fullagar et al., 2015). Interestingly, insomnia has been shown to be common in wheelchair sports athletes, and male WB players are more prone to suffer from insomnia than the overall population. Downregulation of core body temperature is critical for peaceful sleep, and deficits in the autonomic and somatic nervous systems, which govern surface blood flow and perspiration, may impede this process in PPDs. Many players train after daily work activities, and practice sessions are likely to end in the evening. Thus, core body temperature may still be elevated at bedtime (Tsunoda et al., 2017).
Additional explanations for insomnia in wheelchair athletes have been proposed. Individuals who have abnormalities of the spine and/or lower limbs regularly wake to shift posture due to discomfort or to prevent pressure sores. Impaired sleep may have a profound effect on WB players. Intervention research found that young adults’ energy and vigor levels declined with nighttime sleep restriction and were restored after 2 days of adequate sleep (Tsunoda et al., 2017). Extending nighttime sleep duration, while beneficial to athletes’ emotional and physical health, is not without certain potential adverse effects in PPDs. Prolonged sleep may increase tissue damage from pressure ulcers in individuals who have trouble shifting positions while sleeping and who may have impaired protective sensory function. According to another study, short naps had a favorable effect on lowering feelings of fatigue and boosting sprint performance in the setting of partial sleep deprivation (Mutsuzaki et al., 2018). Short sleep periods may also be beneficial for wheelchair athletes while decreasing the risk of pressure ulceration (Tsunoda et al., 2017).
DISCUSSION
Engaging in regular sporting and exercise activities is critical for mental and physical well-being, regardless of whether an individual is physically disabled or able-bodied. WB is a sport that it offers PPDs a variety of scientifically-proven health advantages, and WB categorization systems allow PPDs with varying levels of disability to engage equitably in the sport. WB is extremely competitive at the highest levels but is also widely played recreationally, allowing athletes of all skill levels to reap some of the previously discussed benefits (social, physical, and psychological). WB enhances cardiovascular fitness, improves blood lipid levels, and supports shoulder and trunk muscle strength and endurance. WB has been shown to increase social relationships, improve mental health, and bolster self-esteem. PPDs associate feelings of empowerment with recreational sports, and WB can have profound effects on the QoL for athletes who may have built their social networks around the sport (Ashton-Shaeffer et al., 2001).
The structure, size, and weight of a wheelchair can all have an impact on an athlete’s performance, and newer generation WB wheelchairs are remarkably technically advanced. WB is associated with a variety of injuries, particularly to the upper extremity. The demands of wheelchair propulsion during sport and day-to-day living and the weight-bearing necessary for transfers and everyday activities places particular strain on the shoulder girdle. WB can also result in wrist, elbow, spine, and leg injuries. Proper warm-up, aerobic conditioning, and utilization of sport-specific equipment can help prevent injuries. As athletes display an HR equivalent to values over the anaerobic threshold for the majority of the playtime, WB commands a high cardiovascular load. As a result, WB necessitates high-intensity training to prepare for the physiological requirements of the game. WB match-play is characterized by high-intensity intermittent exertion, and accelerative wheeling sprint capacity from a standstill and over short distances may be crucial for game performance. Muscle strength and power are thus predictors of success in WB.
CONCLUSION
In conclusion, WB is a complex, highly-physical sport that is enjoyed by many PPDs throughout the world. A large body of research exists delineating cardiovascular and mental health benefits, injury risk, and performance-enhancing strategies in the sport. Future research and policies aimed at expanding sport participation in PPDs should aim to expand upon this body of work so that future generations can continue to enjoy this engaging and beneficial sport.