INTRODUCTION
Stroke can arise from either a blockage in the blood vessels of the brain, causing ischemic stroke, or the bursting of brain blood vessels, leading to hemorrhagic stroke where blood seeps into the brain tissue (Knight-Greenfield et al., 2019). According to a study published in 2021, stroke was identified as the second most common cause of death, and its prevalence has been observed to rise compared to the past (GBD 2019 Stroke Collaborators, 2021). The majority of stroke survivors encounter hemiplegia, which is characterized by paralysis affecting one side of the body (Sathian et al., 2011). The paralyzed side of the body exhibits muscle weakness and limitations in range of motion (ROM) (Beebe and Lang, 2009; Bohannon, 2007). These physical impacts also affect functional factors such as balance and gait (Gama et al., 2017; Hayes et al., 2016). Furthermore, these physical and functional effects contribute to psychological factors, such as depression, in stroke patients (Robinson and Jorge, 2016). Therefore, stroke patients engage in various exercise rehabilitations to return to daily activities.
Vibration-based rehabilitation is one of the interventions provided to stroke patients (Liu et al., 2023). Vibration, notably through interventions such as whole-body vibration, has been applied to stroke patients in rehabilitation (Khalifeloo et al., 2018; Kim and Lee, 2021). Whole-body vibration has the advantage of being able to perform additional exercises along with the benefits of vibration (Han et al., 2019; Jung et al., 2020; Kim and Lee, 2021). However, a recent development is the vibration foam roller, which combines vibration with a foam roller. The vibration foam roller has shown advantages in increasing hamstring flexibility compared to a non-vibration foam roller (Lim and Park, 2019). Another study found that using a vibration foam roller on the hamstrings led to increased activation of the antagonistic muscles (Lim et al., 2019). Additionally, the vibration foam roller has been reported to enhance lower limb ROM in both healthy individuals and athletes (Park et al., 2021b).
Whole-body vibration has been reported as effective and safe for treating spasticity in stroke patients (Zhang et al., 2023). In another study, whole-body vibration rehabilitation demonstrated positive effects on the balance and gait of stroke patients (Yin et al., 2023). However, in clinical practice, the use of whole-body vibration is limited by its impracticality for portable use and availability only in specific facilities. On the other hand, the vibration foam roller has primarily been researched in healthy individuals and athletes. While vibration has shown positive effects on stroke patients, there is a lack of research on the vibration foam roller specifically for stroke patients. Therefore, the purpose of this study was to investigate the immediate effects of vibration foam rolling on dorsiflexion ROM, balance, and gait in stroke patients.
MATERIALS AND METHODS
Participants
This study included 30 patients diagnosed with stroke who were undergoing inpatient treatment at a rehabilitation hospital in Gwangju. The inclusion criteria were individuals with a score of 24 or higher on the Korean Mini-Mental State Examination and the ability to gait independently for a distance of more than 10 m. Exclusion criteria included individuals with orthopedic and musculoskeletal disorders, as well as those diagnosed with osteoporosis. The study was conducted with the approval of the Institutional Review Board (IRB) of Nambu University (IRB No. 1041478-2023-HR-005), and all participants provided voluntary informed consent before the study commenced.
Experimental procedure
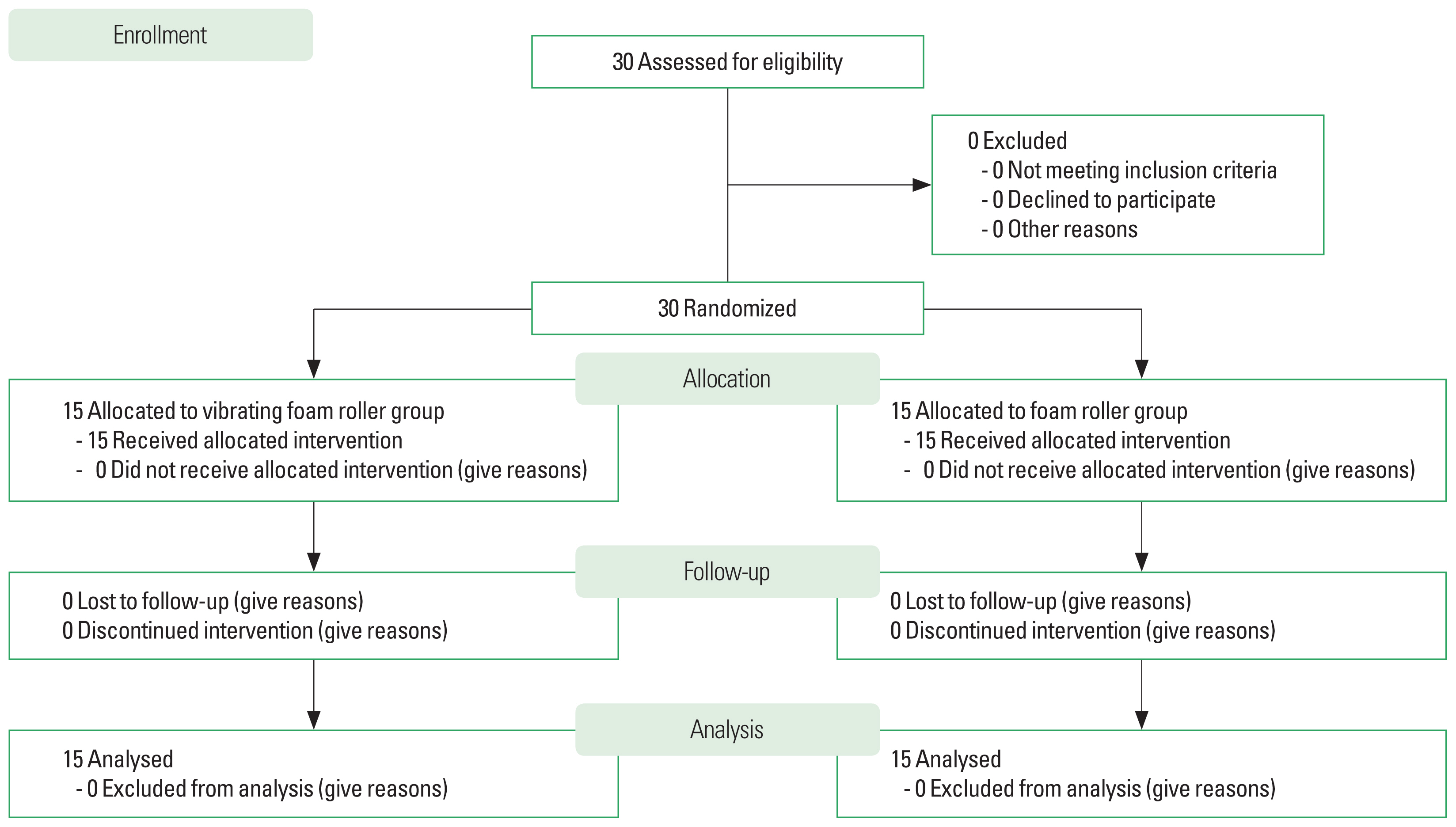
This study was conducted from June 2023 to August 2023, spanning 3 months. Participants were randomly assigned to two groups, and the researchers measured their general characteristics. Before implementing the intervention, evaluative assessments of dorsiflexion ROM, balance, and gait were conducted by the researchers. Subsequently, a single intervention session was immediately administered to both groups. Postassessments were then conducted immediately after the intervention, under the same conditions as the pre-assessments. The foam roller exercise program was performed by a physical therapist holding a master’s degree with over 10 years of clinical experience. Measurements were conducted by a physical therapist with a master’s degree and more than 3 years of clinical experience. The experimental procedure of this study is presented in Fig. 1.
General characteristics collection
General characteristics were collected from participants’ latest data in the electronic medical record (EMR). The EMR data collection was conducted with approval obtained from the IRB, participants, or their guardians prior to study participation. Additionally, to represent the functional level of stroke participants in general characteristics, balance and walking abilities were further evaluated. Balance was assessed using the Berg balance scale (BBS). A BBS score of 49 points or below indicates a risk of falls in stroke patients (Simpson et al., 2011). Walking ability was assessed using the functional ambulation category (FAC). The FAC is a reliable and valid assessment tool for stroke patients (Mehrholz et al., 2007). A score of 4 on the FAC indicates the ability to walk independently on flat surfaces but requiring assistance from a supervisor on stairs, inclines, uneven surfaces, etc. The BBS and FAC assessments were conducted by physical therapists.
Dorsiflexion ROM
This study evaluated the participants’ dorsiflexion ROM using the dorsiflexion lunge test, a reliable method for assessing dorsiflexion ROM in stroke patients (Simondson et al., 2022). The paralyzed-side foot of the participants was positioned in front, and they were instructed to lunge forward until their knee touched the wall, ensuring that the heel remained in contact with the floor at all times. The foot should move away from the wall just enough for the knee to lightly touch it, and the heel should remain in contact with the floor. The distance between the wall and the toes was measured.
Balance
This study utilized the smart balance device (Neofect, Sungnam, Korea) to assess participants’ balance by measuring the limits of stability (LOS). For LOS measurement, participants stood on the platform and faced the front screen. The center of pressure point displayed on the screen was moved in eight directions to measure LOS. The center of pressure was moved in one direction for 10 sec, and the total moved area was used in the study. Both feet were required to be on the platform, and if a participant lifted their foot from the platform, the test was repeated from the beginning.
Gait
This study evaluated the participants’ gait using the Timed Up and Go (TUG), a reliable method for assessing gait in stroke patients (Flansbjer et al., 2005). For the TUG test, participants started from a seated position in a chair with a backrest, walked a distance of 3 m to a turning point upon a signal, and then returned safely to the chair, where the time taken was measured.
Vibrating foam roller group
The vibrating foam roller (Hyperice, Irvine, CA, USA) used in this study’s exercise program has dimensions of 30 cm in length, 15 cm in diameter, and weighs 1.6 kg. Participants were subjected to vibration at 28 Hz. The exercise program, designed based on previous research, consisted of a total of three movements (Park et al., 2021a). Each leg performed exercises for 4 min, followed by a 1-min rest, resulting in a total exercise time for both legs. Each set of exercises lasted 10 min, and the total exercise duration was 30 min. The exercise program is detailed in Table 1.
Foam roller group
This study’s foam roller group performed the same exercise program as the vibrating foam roller group. However, throughout the exercise program, the vibrating foam roller employed by the foam roller group had its vibration feature deactivated.
Data analysis
This study included 30 participants (15 per group) based on calculations considering an effect size of 1.42 from previous research, a power of 0.8, and a dropout rate of 10% (Park et al., 2021a). Data were collected from Outcome Measurements, assessed 3 times and averaged for analysis. Statistical analysis was performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). Nonparametric tests were adopted due to the data not satisfying the normality assumption. Homogeneity tests between groups were conducted for the general characteristics of the research participants. To examine intergroup differences, Mann-Whitney U-tests were applied to analyze prepost difference values. For intragroup differences, Wilcoxon signed-rank tests were used for prepost comparisons. The statistical significance level was set at 0.05.
RESULTS
Characteristics of participants
The study included a total of 30 subjects (Table 2). The vibrating foam roller group and the foam roller group were randomly divided into 15 subjects, and there were no significant differences in the general characteristics of the subjects (P>0.05).
Dorsiflexion ROM
The within-group change in dorsiflexion ROM after the intervention was significant for both the vibrating foam roller group and the foam roller group (P<0.05). Furthermore, there was a significant difference in dorsiflexion ROM between the vibrating foam roller group and the foam roller group (P<0.05) (Table 3).
Balance
The within-group change in balance after the intervention was not significant for both the vibrating foam roller group and the foam roller group (P>0.05). Furthermore, there was no significant difference in balance between the vibrating foam roller group and the foam roller group (P>0.05) (Table 3).
Gait
The within-group change in gait after the intervention was significant for the vibrating foam roller group (P<0.05), whereas it was not significant for the foam roller group (P>0.05). Furthermore, a significant difference in gait was observed between the vibrating foam roller group and the foam roller group (P<0.05) (Table 3).
DISCUSSION
This study investigates the effects of applying a vibrating foam roller to stroke patients, examining its impact on dorsiflexion ROM, balance, and gait depending on the presence of vibration. The results reveal that the vibration foam roller group showed significant differences in dorsiflexion ROM and gait after the intervention, while the foam roller group exhibited a significant difference only in dorsiflexion ROM. In comparisons between the vibration foam roller group and the foam roller group, significant differences were observed in dorsiflexion ROM and gait. However, there were no significant differences in balance, both before and after the intervention, as well as in the comparisons between the two groups.
In this study, both groups performed the same foam rolling and exercise program. Vibration was only added to the vibrating foam roller group. The use of a foam roller has demonstrated results consistent with previous studies, indicating a reduction in muscle stiffness and an increase in ankle flexibility, contributing to improved ROM (de Benito et al., 2019). This implies that the effective relaxation of muscles and fascia through foam roller application has positively influenced dorsiflexion ROM, resulting in significant differences within the groups (Dębski et al., 2019). While earlier studies reported no significant difference in ROM between foam rollers and vibrating foam rollers (García-Gutiérrez et al., 2018), our study revealed a significant difference between the vibration foam roller group and the foam roller group. Other previous research comparing vibrating foam rollers and regular foam rollers in stroke patients showed significant differences between the experimental and control groups, aligning with our findings (Park et al., 2021a). These effects are attributed to the enhancement of ROM through increased blood circulation induced by vibration stimulation (Veqar and Imtiyaz, 2014). In previous studies, vibration has been shown to influence physiological processes in both the circulatory and nervous systems (Games and Sefton, 2013). Analysis of blood samples following exercise combined with vibration revealed physiological effects (Lin et al., 2015; Kulich et al., 2022). Therefore, due to the additional benefits of vibration, it is believed that the group using the vibrating foam roller demonstrated more significant changes compared to the group without vibration.
Due to the increased flexibility of the ankle, dorsiflexion during the sit-to-stand phase, where the trunk bends forward, was likely facilitated (Sadeh et al., 2023). Subsequently, this heightened flexibility may have served as a foundation for progression during the push-off phase of walking and aided in changing direction at the 3-m point, potentially resulting in a significant improvement in the TUG test (Agathos et al., 2023; Cho and Park, 2020). Additionally, considering the impact of vibration stimulation on cortical activation in the cerebral cortex of stroke patients, it is speculated that no significant results were observed in the control group. Previous studies have demonstrated cortical activation in the vibration stimulation group, whereas no changes were observed in the control group (Lee et al., 2020).
Balancing abilities play a crucial role in postural control and stabilization, serving as an indicator of an individual’s capacity to perform activities independently and predicting favorable outcomes (Makizako et al., 2015). Previous studies have explored exercises targeting the trunk to enhance postural control in stroke patients (Salgueiro et al., 2022). However, it is speculated that the exercise program in this study, conducted as a single session, might have lacked the duration and intensity necessary for a significant improvement in balance abilities. In this study, we used the area of the LOS as a measure of balance. When assessing stroke patients, the notable tendency is for the LOS area not to be centrally located but often skewed towards the nonparalyzed side. While the LOS area is significant, future research should also consider qualitative assessments to ensure that the LOS area can be centered in subsequent evaluations.
This study has several limitations. First, the duration of the exerciser program was relatively brief, consisting of a single session. Nevertheless, our findings can lay the groundwork for future investigations exploring long-term changes. Second, the relatively modest sample size might limit the ability to assess the impacts of the vibrating foam roller in relation to the severity of stroke lesions or motor impairments. Future studies may need to consider variations by including a more diverse range of patients with varying degrees of stroke lesions or motor impairments.
In conclusion, this study confirmed that a single-session vibrating foam roller exercise program improves dorsiflexion ROM and gait in stroke patients. Further studies with extended exercise program durations are needed to address limitations and explore long-term effects.