Finger exercise with keyboard playing in adults with cerebral palsy: A preliminary study
Article information
Abstract
The purpose of this study is to examine the effects of Therapeutic Instrument Music Performance (TIMP) for fine motor exercises in adults with cerebral palsy (CP). Individuals with CP (n = 5) received a total of twelve, 30-min TIMP sessions, two days per week for six to nine weeks. Pre- and post-Music Instrument Digital Interface (MIDI) data were used as a measure of hand function. Pre-velocity was significantly different from the normative data obtained from typical adults (n = 20); however, post-velocity did not yield significance, specifically in the second and fifth fingers, indicating improvement in hand function for the adults with cerebral palsy. The finding implies that TIMP using keyboard playing may effectively improve manual dexterity and velocity of finger movement. Based on these results, future program development of instrumental playing for adults with CP is called for to enhance both their independent living skills and quality of life.
INTRODUCTION
Cerebral palsy (CP) is a nonprogressive motor disorder resulting from injury to or abnormal development of the brain. It manifests as various problems in movement, posture, and other behavioral functions. The types of motor impairment associated with cerebral palsy include: dystonia, ataxia, and spasticity (Bax et al., 2005). Depending on the location of the brain injury or impairment and its degree of severity, additional disabilities may be evidenced in the motor, intellectual, sensory, communication, and behavioral domains (Kim and Han, 2008; Rosenbaum et al. 2007). In particular, upper limb involvement in spastic CP varies from mild clumsiness to fixed muscle contractures preventing active extension of the elbow, wrist, or fingers, while dyskinetic CP presents involuntary, uncontrolled movements (Manske, 1990).
Individuals with cerebral palsy have to utilize extra strength in order to move their upper extremities and have extensive difficulty controlling these movements due to high muscle tension (Barrett et al., 2010; Lee and Song, 2009). Limitations in fine motor skills make independent living problematic if not impossible and negatively impact everyday functioning in terms of educational, professional, and social activities. However, since fine motor problems are less overt than gross motor problems, and hence more difficult to study, less attention has been paid to fine motor problems in the research (Arner et al., 2008; Beckung and Hagberg, 2002).
Most studies on the use of physical therapy with individuals with cerebral palsy deal with the efficacy of repeated physical training and its restorative effect. This is supported by neuro-plasticity theory (Blanton et al., 2008). Overall, conventional physical therapy approaches for cerebral palsy focus on the application of training interventions developed in reference to normal motor development. This is because in the case of cerebral palsy, the motor development lacks normal motor development process and pattern due to a dysfunctional central nervous system and a delayed synthesizing function (Ketelaar, 1998; Sorsdahl et al., 2010). This kind of intense rehabilitation training is conventionally provided during early childhood; therefore, adults with cerebral palsy have less chance and opportunity to receive rehabilitative interventions. Studies show that more than 50% of young adults with CP withdraw from health services despite their health problems (Bax et al.,1988) and self-reports of multiple musculoskeletal difficulties and pain (Andersson and Mattson, 2001). Therefore, effective upper limb rehabilitative training that motivates adults with cerebral palsy to remain in treatment is greatly needed.
Among the many interventions available for physical rehabilitation, neurological music therapy is one of the few clinical interventions using music as a major rehabilitative cue to induce various brain and motor responses. There are ongoing studies on the use of rhythm auditory stimulation (RAS) to treat gait problems. Rhythm auditory stimulation is a technique that facilitates auditory-motor synchronization in the reticulo-spinal tract. An auditory cue is used to elicit a desirable motor movement and muscular activation in a step-by-step formation until a complete target movement is elicited (Thaut, 2005; Thaut and Abiru, 2010).
Therapeutic Instrument Music Performance (TIMP) technique uses instruments to reinforce functional motor patterns, and the instruments used usually involve percussive instruments which do not require any previous music skills. Selection of instruments, application of various playing techniques, and adaptation of playing posture are the variables associated with bringing out effective changes in finger dexterity, independent manipulation, coordination, range of mobility, palmar grasp, and pincer grasp (Thaut, 2005). In other words, the instruments are not used to produce musical output, but to facilitate movement associated with non-musical rehabilitative purposes (e.g., placing various sizes of drums at different heights for the player in order to induce expanded range of arm movement. The player will extend the arm to play the drum at different spatial locations).
For fine motor skill training, TIMP usually uses the keyboard as its main rehabilitative intervention. The literature suggests that the effectiveness of keyboard training can be measured via a computer data analysis system called Musical Instrument Digital Interface (MIDI). This software provides quantitative measures of the rehabilitative intervention. In previous research, MIDI was used to detect the pressing intensity and playing velocity of older adults with osteoarthritis. The data collected by MIDI show the accuracy of the participants’ pressing as well as their frequency and timing, and show that MIDI keyboard playing is an effective rehabilitative tool (Zelany, 2001). Recently, research interest in utilizing music playing for upper limb rehabilitation has been rising, and the use of keyboards and electronic drums have been shown to be statistically effective in improving movement patterns and quality of motion (Schneider et al., 2007). These results have led to comparative studies on music interventions which show that music is an effective rehabilitative intervention for upper limb functioning (Schneider et al., 2010).
In other studies on TIMP, positive results were found on the pincer grasp, dexterity, and functional skills, however, most of these studies involved stroke patients (Altenmuller et al., 2009; Schneider et al., 2007; Yoo, 2009). There are very few studies on TIMP with individuals with cerebral palsy. What research does exist focuses on younger children with cerebral palsy leaving adults with cerebral palsy in urgent need of research on effective rehabilitation and treatment strategies (Han, 2011).
According to the research, keyboard playing not only provides pleasure from making audible music, but also motivates individuals to participate in rehabilitation by using their affected and intact hand functions. These are crucial factors in treating adults with cerebral palsy. As a result, keyboard playing can be an effective intervention for restoring behavioral functioning and preventing motor regression. In this study, the keyboard was used as a major rehabilitative intervention and the MIDI variable of velocity was measured before and after the intervention to detect the intervention’s effect. The study also examined changes in the participants’ finger pressing force. Finally, the data were compared to outcomes for a group of healthy adults in order to assess the participants’ proximity to normal functioning following the intervention.
Research question 1: Is there a difference in the velocity of the finger after TIMP training with a keyboard for adults with cerebral palsy?
Research question 2: Will the difference between velocity scores of adults with CP and healthy adults be diminished after TIMP training?
MATERIALS AND METHODS
Participants
The participants were recruited from a rehabilitation ward in a university medical center located in Seoul (Table 1). A total of five participants were selected based on the following inclusion criteria: 1) adults ages 20 to 39 with cerebral palsy and 2) no difficulties in verbal communicative skills. Participant A was diagnosed with dyskinetic type cerebral palsy and dysarthria, participants B and C were diagnosed with spastic diplegia, participant D had Spastic hemiplegia, and participant, E had Spastic type cerebral palsy. All the participants were able to sit and participate in keyboard playing without any physical assistance. All the research procedures were reviewed and approved by the university research review board (IRB No. 2012-07-03). Participants were given verbal descriptions of what their participation would entail and were informed of the consent procedures and their rights as participants. They signed the consent form upon agreeing to participate.
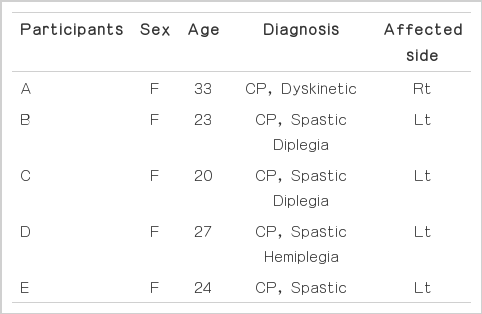
Characteristics of participants
The study was initially designed to examine changes in hand function by comparing the pre and post scores of conventional measurement test tools, but it was agreed that the short-term repeated hand function test would not be feasible for the participants considering their diagnoses and ages.
Measurement tool
Each of the five individuals participated in measurement of hand function before beginning training with the keyboard. Hand function was measured using MIDI of their key pressing force. For the MIDI program, Cubase 6 was used and the velocity was measured before and after keyboard training.
Procedure
Each training session lasted for 30 min and two sessions were held each week for a maximum of nine weeks. The training was administered in a private space at the medical center, and all training sessions were conducted individually. The posttest was administered on the last day of the intervention.
TIMP training program
The music used for training was selected based on the preference of the participants, taking the melodic line as the main theme to be played repeatedly with their fingers. In the first half of the training, repeated pressing (finger no. 1–5), sequential playing (ascending 1, 2, 3, 4, 5; descending 5, 4, 3, 2, 1), and simultaneous pressing (1.2, 1.3, 1.4, 1.5; 3.4.5, 4.5, 3.5) were measured (Fig. 1).

Numbering of fingers.
In the second half of the training, extended melody was played in order to maximize the range of motion among the fingers. Warm-up activity with music was applied before the TIMP intervention in order to facilitate relaxation of the gross motor tension. In the initial stage, the TIMP intervention focused on playing fingers individually; however, the treatment transitioned into playing using all of the fingers.
Data analysis for keyboard playing
The data for this study was collected via the Cubase 6 MIDI program focusing on the quantified measures of velocity. The velocity of keyboard playing indicates the intensity of key strike and changes in the pre- and post-intervention measures represent improvement. Data were collected from five trials; however, the minimum and maximum figures were excluded leaving data for 3 trials. The maximum velocity score of Cubase 6 was set to 127. Descriptive statistics were gathered to examine pre and post scores of individual fingers, and in order to compare the healthy group and the experimental group. The Mann-Whitney test was used for analysis (P<0.05).
Normative data for keyboard playing for healthy adults
In order to compare and contrast the fine motor skills of outpatient adults with cerebral palsy with normative data, 20 healthy adults (all female) without any music background participated in the keyboard playing in order to draw normative data using MIDI. Volunteers to play MIDI keyboard were recruited from two different universities and all participants signed the written consent form. The collected data were used to compare the performance task with the affected hand for adults with cerebral palsy. The assessment protocol was identical to the one used for adults with cerebral palsy.
RESULTS
Effect of TIMP training analysis
The MIDI scores of pre and post TIMP training for individual fingers are shown in Table 2. The mean of the individual fingers improved in the post training measurement. However, there were no significant differences. Among the fingers, the biggest improvement was shown in the fourth finger (pre-post difference 8.5), and the changes shown in all five fingers were consistent.

Comparison of MIDI scores for individual fingers after TIMP training
Comparative analysis with data from healthy adults
In order to compare the performance task of the affected upper limb of adults with cerebral palsy, the data for nondominant hand healthy adults were gathered using MIDI keyboard playing. Healthy adults in their 20s without any music background participated and their MIDI data are shown in Table 3. A comparison of the data collected from healthy adults and adults with cerebral palsy is shown in Table 4.

MIDI data on dominant and nondominant hands of healthy adults

Comparison of affected hand of adults with CP and nondominant hand of healthy Adults
The MIDI data of the healthy adults’ nondominant fingers were individually analyzed. The results showed that there were significant changes in the first finger (P=0.035), third finger (P=0.017), and fourth finger (P=0.049) after the TIMP training. However in the second finger (P=0.096) and fifth finger (P=0.077) there was no significant difference (Table 5). One can interpret that the non-significant results of this study imply that there was less variability in the performance of the healthy adults than the adults with cerebral palsy. This suggests that the velocity of key pressing force in the adults with cerebral palsy increased to a significant level. Therefore, one can conclude that the second and fifth fingers improved to a greater degree among all the fingers as continuous training was provided to the adults with cerebral palsy.

MIDI data on CP adults’ and healthy adults’ individual fingers
DISCUSSION
This study showed that the participants’ upper limb function, specifically finger pressing force, was increased and finger manipulation was improved in terms of sequential movement of fingers. When we compare the pre and post MIDI data of finger pressing force for adults with cerebral palsy, the positive changes in the entire hand function show that repeated use of fingers facilitated increased pressing force. These results are consistent with those of other studies which examined the effect of finger manipulating interventions (e.g., finger keyboard, games, toys) and finger dexterity (Choi and Kwon, 2005), These results support that keyboard training can be an appropriate and effective intervention for adults with cerebral palsy.
According to the results from the comparison of MIDI scores with healthy adults’ nondominant hands, there were many differences among the fingers. Despite large intersubject variability, three fingers (F1, F3, F4) showed significant improvement in finger pressing force. It has been known that the index and middle fingers are stronger than the ring and little fingers (Dickson et al., 1972; Martin et al., 1996). Statistical significance found in the ring finger may be due to the fact that keypressing movement induced by keyboard playing is associated with increased corticospinal excitability in relation to individual finger movement in terms of both abduction and adduction movements (Carroll et al., 2002). Overall, the findings imply that keyboard playing as a motor skill training method can be an effective finger exercise tool for adults with CP.
Along with the results of previous studies with MIDI keyboard playing, it is meaningful to expand the application to adults with CP due to their limited options for fine motor rehabilitation. Currently, most interventions for the rehabilitation of cerebral palsy involve gross motor areas. The primary reason behind this is to help them learn everyday living skills such as standing up and walking. Due to this priority, research in developing effective interventions for fine motor skills for different types of cerebral palsy is comparatively scarce. Keyboard rehabilitation training is an effective intervention for fine-motor rehabilitation and generates intrinsic motivation to continue participation in music making.
In order to provide consistent MIDI keyboard training normative MIDI data from a substantial sample is required and comparative studies are needed on the MIDI scores obtained from diverse populations. In this study, 20 female nondominant hand MIDI scores were collected and future studies using larger sample sizes will contribute to the validity of the study. Also, in the training of this study, a wrist support pad was used to minimize the spastic tension of the hand elicited when striking the keyboard. The participants were asked to play the ascending and descending melodic lines (F1-F2-F3-F4-F5) to prompt the efficiency in the finger progression. The use of a wrist pad seems to be effective to reinforce the keyboard playing of adults with cerebral palsy.
Overall, the results of this study support the positive effect of keyboard training on the enhancement of fine motor/finger functions for adults with cerebral palsy. Future studies can examine any correlation between finger strength and hand function. Also, future studies can examine the effect of differentiated use of the keyboard for specific motor problems. Lastly, more studies should be administered to examine other benefits of keyboard playing as a rehabilitation tool.
Acknowledgements
This work was supported by the Ewha Global Top 5 Grand 2012 of Ewha Womans University, Seoul, Korea.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.