A study of the relationship among fear-avoidance beliefs, pain and disability index in patients with low back pain
Article information
Abstract
This study was conducted in order to determine the relationship among fear-avoidance beliefs, pain and disability index in patients with low back pain as well as to identify factors having an influence on fear-avoidance beliefs, pain and disability index. The subjects used in this study were 55 patients with low back pain. All subjects completed a fear-avoidance beliefs questionnaire (FABQ) which was divided into two subscales, FABQ for physical activity (FABQ-P) and FABQ for work (FABQ-W), Visual Analog Scale (VAS), Oswestry Disability Index (ODI) and Roland Morris Disability Questionnaire (RMDQ). In correlation analysis, FABQ-P appeared to show significant correlation with FABQ-W, FABQ-total, VAS and RMDQ, and all variables showed significant correlation with each other. Findings of this study suggest that screening for fear-avoidance beliefs may be useful for identification of patients at risk of psychosocial problems as well as pain intensity and physical impairment.
INTRODUCTION
Low back pain (LBP) is a common clinical problem and the lifetime prevalence of back pain is 60–80%. LBP has become a major medical, social and economic problem (Waddell, 1993). The main causes of LBP has the spinal structures including inter-vertebral discs, facet joints, vertebral bodies, ligaments, or muscles could be an origin of back pain, biomechanical factors because decrease of functions of the musculoskeletal system (Graves et al., 1990) and psychological factors such as fear, anxiety, depression, and a sense of helplessness often contribute to the development and maintenance of chronic pain and associated disability (Samwel et al., 2006).
Pain is one of the most powerful aversive drives in animals and humans, is closely allied to fear. Pain has been described using a variety of conceptual definitions among which pain-related fear, fear of movement, and kinesophobia are the most commonly used (Lundberg et al., 2011). In a subset of patients with low back pain, development of fear resulted in avoidance of actual or perceived pain-generating physical activities and led to worsening performance and recovery after injury (Waddell et al., 1993). The fear of pain is an important aspect in patients’ disability, which needs to be addressed in order to achieve a successful outcome (Lundberg et al., 2011).
Pain-related fear is part of the Fear-Avoidance Model (Lethem et al., 1983). The Fear-Avoidance Model has been used to explain the development of unfavorable pain experiences and behaviors (Vlaeyen et al., 1999). Troup et al. (1987) outlined the most specific “fear-avoidance model of exaggerated pain perception” in chronic low back pain. Fear-avoidance beliefs of LBP patients predicted disability in daily or occupational activity, treatment outcome, and patients’ return to work after a functional restoration program (Pfinqsten et al., 2000). High scores on the Fear-Avoidance Beliefs Questionnaire (FABQ) (Waddell et al., 1993), a validated two-part questionnaire, which examines the role of fear in physical activity and work, have been attributed to the maintenance of both chronic pain and pain-related disability (Basler et al., 2008).
Therefore, the purpose of this study was to determine the relationship among fear-avoidance beliefs, pain and disability index in patients with low back pain as well as to identify factors having an influence on fear-avoidance beliefs, pain and disability index.
MATERIALS AND METHODS
Subjects and treatments
A total of 55 patients with low back pain were included as subjects in this study. The subjects were provided with a full explanation of the experimental procedure and all subjects provided written consent signifying voluntary participation. The subjects were inpatients at K hospital in Seoul city in Korea, from May to September in 2012. The criterion for selection was diagnosis with chronic LBP by a physician. Exclusion criteria were: 1) neurological problem such as stroke, 2) rheumatoid arthritis, 3) cancer, 4) pregnant, and 5) hypertension.
Fear-avoidance beliefs were measured using a modified form of the FABQ, a 16-item, self- report scale, which focuses specifically on patient’s beliefs about how physical activity and work affects their pain. The FABQ Physical activity (FABQ-P) assessed attitudes and beliefs related to general physical activities (four items, range 0–24) and the FABQ Work (FABQ-W) assessed attitudes and beliefs related to occupational activities (seven items, range 0–42). Each item is scored from 0, “do not at all agree” to 6 completely “agree”. For both subscales, a low score indicates low fear-avoidance beliefs, and a score of 14 or more on the FABQ Phys indicates strong fear-avoidance beliefs (Waddell et al., 1993).
The intensity of LBP was usually evaluated using a visual analogue scale (VAS). A 10 cm horizontal line ranged from no pain to severe pain, and numbered from 0 to 10 (0=no pain, 5=moderate pain, 10=worst pain). The patient marked the point that he felt represented his perception of his current state.
The Disability index of LBP was evaluated using the Roland Morris Disability Questionnaire (RMDQ) and the Oswestry Disability Index (ODI). The RMDQ is a measure used in assessment of self-reported disability due to low back pain. The RMDQ consists of 24 items. Each item is qualified with the phrase “because of my back pain”. The scores range from 0, indicating no disability, to 24 indicating severe disability (Roland and Fairbank, 2000). The modified ODI is a 10-question condition specific measurement of pain and disability for individuals with LBP. Each question is scored from 0 to 5 and summed for determination of total score, which is multiplied by 2 and expressed as a percentage (Fairbank et al., 1980).
Statistical analyses
All statistical analyses were performed using the SPSS statistical package, version 16.0. The general characteristics and characteristics of low back pain are presented as the frequency and percentage, and the average and standard deviation are also provided. The t-test was used for analysis of the difference in the FABQ, pain and disability index. The Pearson’s correlation coefficient was used to examine the correlation among FABQ, pain and disability index. Results were considered significant at P<0.05.
RESULTS
Table 1 lists the general characteristics of the subjects. There were 32 (58.2%) males and 23 (41.8%) females. The averages for age, height and weight were 46.4 yr, 166.7 cm, and 66.6 kg, respectively. Table 2 lists the low back pain characteristics of the subjects. In recurrence, 33 (60.0%) subjects had first occurrence and 22 (40.0%) subjects had recurrence. Thirty seven (67.3%) subjects had radiating pain and 18 (32.7%) subjects did not. Twenty two (40.0%) subjects had pain of unknown cause, 20 (36.4%) subjects had accidents, six (10.9%) subjects had disease, and seven (12.7%) subjects had other, respectively. Fifteen (27.3%) subjects underwent one more surgery and none surgery was 40 (72.7%) subjects. Thirty three (60.0%) subjects were taking medication and 22 (40.0%) subjects were not taking medication. Regarding duration, nine (16.4%) subjects were acute (within six weeks), 10 (18.2%) subjects were sub-acute (6–12 weeks), and 36 (65.5%) subjects were chronic (more than 12 weeks).

General characteristics of the subjects (N= 55)
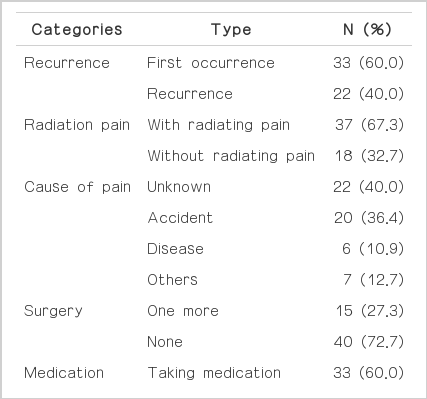
Low back pain characteristics of the subjects (N= 55)
Table 3 lists the descriptive characteristics of subjects for measures FABQ, VAS, RMDQ, and ODI. The mean score of FABQ-total was 39.2. The average scores for FABQ-P, FABQ-W, VAS, RMDQ, and ODI were 15.6, 24.1, 5.7, 10.7, and 32.5, respectively.
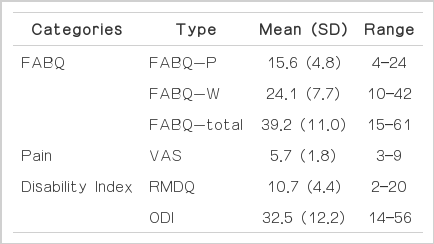
Descriptive characteristics of subjects for measures FABQ, VAS, RMD, and ODI (N= 55)
Table 4 lists the correlation between FABQ, VAS, RMDQ, and ODI. FABQ-W (r=0.496, P=0.000), FABQ-total (r=0.794, P= 0.000), VAS (r=0.320, P=0.017), and RMDQ (r=0.372, P= 0.005) showed significant correlation with FABQ-P. FABQ-total (r=0.918, P=0.000), VAS (r=0.292, P=0.031), RMDQ (r= 0.433, P=0.001), and ODI (r=0.376, P=0.005) showed significant correlation with FABQ-W. VAS (r=0.338, P=0.012), RMDQ (r=0.455, P=0.000), and ODI (r=0.338, P=0.001) showed significant correlation with FABQ-total. RMDQ (r=0.530, P= 0.000) and ODI (r=0.494, P=0.000) showed significant correlation with VAS. ODI (r=0.592, P=0.000) showed significant correlation with RMDQ.
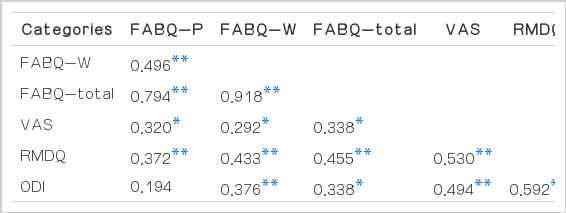
Correlation between FABQ, VAS, RMDQ, and ODI (N= 55)
DISCUSSION
Pain and pain disability are not only influenced by organic pathology, if found, but also by biological, psychological and social factors. Fordyce et al. (1982) described how pain behavior may also result from avoidance learning. Avoidance refers to “the performance of a behavior which postpones or averts the presentation of an aversive event”. In the case of pain, a patient may no longer perform certain activities because he/she anticipates that these activities increase pain and suffering.
The concept of fear-avoidance has offered an enticing model which appears to account for why some people develop dysfunctional pain problems (Linton et al., 2000). The purpose of this study was to determine the relationship among fear-avoidance beliefs, pain and disability index in patients with low back pain as well as to identify factors having an influence on fear-avoidance beliefs, pain and disability index. In this study, Fear-avoidance beliefs were measured using a modified form of the FABQ and the intensity of LBP was usually evaluated using a VAS. The Disability index of LBP was evaluated using the RMDQ and the ODI.
Pain sensitivity and intensity are associated with physical functional status. Clauw et al. (1999) suggested that an individual’s experimental pain threshold is associated with baseline functional status and caused pain. George et al. (2006) reported that fear-avoidance beliefs about work and temporal summation of evoked thermal pain had a significant influence on pain related disability. These factors should be considered as potential outcome predictors for patients with work-related low back pain. In this study, FABQ-P appeared to show significant correlation with FABQ-W (r=0.496, P=0.000), FABQ-total (r=0.794, P=0.000), VAS (r=0.320, P= 0.017), and RMDQ (r=0.372, P=0.005). FABQ-W, FABQ-total, VAS, and RMDQ variables showed significant correlation with each other.
Cai et al. (2007) who studied correlates of self-reported disability using MODQ (Modified Oswestry Low Back Pain Disability Questionnaire) in patients with low back pain, reported that MODQ score in patients with low back pain showed significantly correlation with pain intensity (P=0.000) and FABQ-W (P=0.007). However, the MODQ score did not show significant correlation with FABQ-P (P=0.37). In this study, the ODI score showed significant correlation with FABQ-W (r=0.376, P=0.005), FABQ-total (r=0.338, P=0.011), VAS (r=0.494, P=0.000), and RMDQ (r=0.592, P=0.000). However, the ODQ score did not show significant correlation with FABQ-P (r=0.199, P=0.146).
Basler et al. (2008) studied fear-avoidance beliefs, physical activity and disability in elderly individuals with chronic low back pain and healthy control subjects. In the patient group, fear-avoidance beliefs, pain intensity and age predicted functional capacity and patients were more fear-avoidant and reported more disability. Camacho-Soto et al. (2012) reported a significant association of fear-avoidance beliefs (P<0.0001) and McGill Pain questionnaire (P<0.0001) in older adults with chronic low back pain with the RMDQ. In this study, the RMDQ showed significant correlation with FABQ-P (r=0.372, P=0.005), FABQ-W (r=0.433, P=0.001), FABQ-total (r=0.455, P=0.000), VAS (r=0.530, P=0.000), and ODI (r=0.592, P=0.000). Caporaso et al. (2012) reported significant correlation of Baseline RMDQ scores with function test scores, except for the sock test (P<0.05). These results show that because of pain, patients have increased pain intensity and limited physical activity. This limitation of physical activity had high self-reported disability index and increased fear-avoidance beliefs by fear of pain, psychological distress, and anxiety. Findings of this study suggest that screening for fear-avoidance beliefs may be useful for identification of patients at risk of psychosocial problems as well as pain intensity and physical impairment.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.