Effects of rehabilitative horse riding on the Sit-to-Stand action of the adolescent with brain lesions
Article information
Abstract
The purpose of this study was to investigate the balance abilities of the adolescent girl with brain lesions by Sit-to-Stand (STS) action analysis before and after the rehabilitative horse riding of 16 week program. The subject aged 16 yr old who had the disabilities of spasticity and hemiplegia was recruited with the consent approval. The equilibrium abilities of the subject were tested by Sit-to-Stand examination with Weight Transfer Time (WTT), Mean Rising Index (MRI), Mean Weight Asymmetry (MWA), Max Trunk Flexion Velocity (MTFV), and Max Trunk Extension Velocity (MTEV). Research was designed by AB single subject study with baseline of 3 times of measurement and rehabilitative horse riding treatments. In the results, the enhancement of the subject’s equilibrium ability was shown from the comparisons between baseline and treatment by the STS test that WTT was 2.37 sec faster, MRI was 6.64 N/kg higher, and MWA was 8.12% lower, and MTFV was 0.57°/sec larger than all those means of baseline. It suggested that the subject showed her enhanced balance ability while in sitting and standing after the rehabilitative horse riding treatments.
INTRODUCTION
The brain lesions refer to the damage on the brain area by injury or disease to be seemed simple, however, complicated to be understood. The types of brain lesion are so variable and the ability to move is affected (http://www.webmd.com/brain/brain-lesions-causes-symptoms-treatments). Also, a brain lesion may affect directly the neuron or indirectly affecting the functions of neuron (http://www.medicinenet.com/brain_lesions_lesions_on_the_brain/page2.htm).
In the case of the individual who has spastic hemiplegia by brain lesions may consist of increased elbow flexion with forearm pronation and increased muscle tone which cause the malfunction in posturing as well as walking (Gage, 2004) The problems of absence of regular gait movement on the side of hemiplegia makes the individual noticeable and particularly problematic in adolescence because the general appearance is so important in the adolescent period (Riad et al., 2011).
Sit-to-Stand (STS) action is an activity that most of human beings should perform many times in their daily lives. Also, STS is a fundamental movement for the balance and directly connects to the skills of walking as well. The basic activity such as STS action in daily living is gradually acquired during early childhood and assured by 7 yr old around (Haley et al., 1992). In the action of STS, the leg muscle and wide ROM of the relative joint are involved considerably to the ability of balance challenge (Hoch et al., 2012; Hylton et al., 2005; Riley et al., 1991). Therefore, the test of STS is an appropriate motor task to identify the functional limitations of the balance ability. Many researchers have examined STS motion analysis targeting the functionally impaired elders (Hesse et al., 1994; Hughes and Schenkman, 1996). Asymmetrical leg load is identified in the stroke patients caused by abnormal muscle utilization and muscle weakness during STS (Eng and Chu, 2002). Furthermore, even healthy populations showed the asymmetrical leg load by exhibiting weaker hamstrings and stronger quadriceps in dominant sides of lower limb (Lanshammar and Ribom, 2011).
Horse riding therapy is treatment strategy to use equine movement for the improvement of functional outcomes such as trunk strength or balance (Cunningham, 2009). Meregilano (2004) explained the therapeutic horse riding was to focus on the stability of trunk, posture, and mobility for the improvement of gait and balance. The effects of horse riding on the gait of the children with cerebral palsy were reported (McGee and Reese, 2009).
Therefore, the subject’s STS action was tested before and after the treatment to examine the effects of rehabilitative horse riding on the balance function which is essential for the walking.
MATERIALS AND METHODS
Subject
A female adolescent girl aged 16 yr old with brain lesions participated in this study as a single subject. The subject was hemiplegic in the right limbs and showed imbalanced walking pattern. The subject’s joints such as spine, hip, knee, and ankle were flexed by the spasm and pelvis was rotated posterior with tilting posture, therefore, stiffness was found in gait pattern which caused easy slip and fall down. The subject’s physical characteristics were shown in Table 1.

Subject’s physical characteristics
Apparatus
The test instruments used in this study were presented in Table 2.
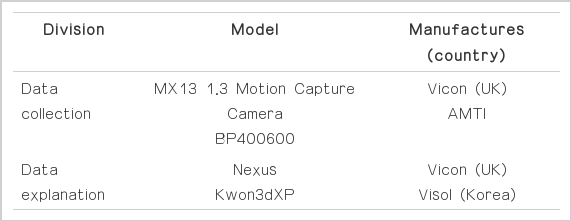
Data collection and analysis apparatus
Experimental procedures
The subject participated in the rehabilitative horse riding training program for once a week and total of 16 weeks. STS motion test was executed for 3 times of baseline period prior to the training program and 3 times of treatment period within the horse riding training program.
Data collection and analysis
For the STS motion test, the subject was dressed by the black sport tights and the refection marks were attached on the joints of 7th cervical, right and left acromion processes, and sacrum. Weight Transfer Time (WTT) of STS motion was measured from sit to the position of peak of weight load on the feet. Means of trunk sway velocity was classified by maximum trunk flexion velocity (MTFV) and maximum trunk extension velocity (MTEV). Mean Rising Index (MRI) was measured by the amount of force created by lower limbs from beginning to end of STS motion. Mean weight asymmetry (MWA) was measured from the position of total weight load on the feet to the position of standing. The equations of MRI and MWA are shown as follows:
RESULTS
In the comparisons between baseline and treatment periods of each variable of STS, WTT was decreased from 5.47±0.81 sec to 3.1±00.33 sec (Table 3 and Fig. 1) and MRI variable was increased from 15.23±0.87 N/kg to 21.87±1.41 N/kg (Table 4 and Fig. 2). MWA was decreased from 36.29±4.09% to 28.17±1.72% (Table 5 and Fig. 3). MTFV was increased from 61.17±8.09°/sec to 62.74±3.86°/sec (Table 6 and Fig. 4). MTEV was increased from 57.36±6.62°/sec to 62.74±3.86°/sec (Table 7 and Fig. 5).
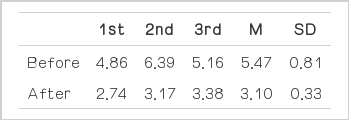
Changes of STS WTT (Weight Transfer Time) (unit: sec)
Change of WTT Mean.
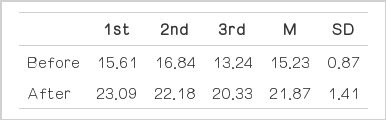
Changes of STS Mean Rising Index (MRI) (unit: N/kg)
Change of MRI Mean.
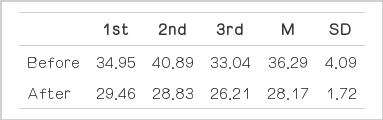
Changes of STS Mean Weight Asymmetry (MWA) (unit: %)

Change of MWA Mean.
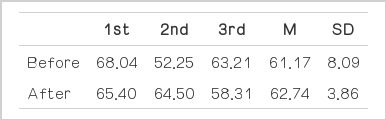
Changes of STS MAX Trunk Flexion Velocity (MTFV) (unit: °/sec)

Change of MTFV Mean.
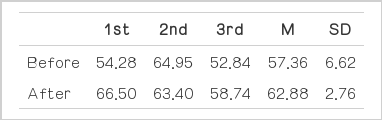
Changes of STS MAX Trunk Extension Velocity (MTEV) (unit: °/sec)

Change of MTEV Mean.
DISCUSSION
In this research, WTT, MRI, MWA, MTFV, and MTEV were examined to identify the changes of movement of STS before and after the rehabilitative horse riding training for the adolescent girl aged 16 yr old who had the brain lesions and those factors were considerable to explain the ability of balance and effectiveness of STS motion which might contribute the subject’s enhanced walking pattern. The decreased WTT is meant as the result of the enhanced balance ability because the high mobility of knee joint was decided by the peak off set which was based on the notes of Hylton et al. (2005) and Hoch et al. (2012), therefore, the balance and stability of the subject could be influenced positively by faster WTT that contributed to the high peak off set. The enhanced MRI could be caused by the increased lower limb force and improved balance function of the trunk usually found in the healthy populations exhibiting stronger quadriceps in the STS movement (Lanshammar and Robom, 2011). The subject of this study showed faster WTT after horse riding training which could contribute to the trunk balance. Symmetry was defined by Herzog et al. (1989) as “perfect agreement of the external kinetics and kinematics of the left and right leg”. Based on their research, the ground reaction force applied to the feet more than 10% difference between two legs from the perfect symmetry could be interpreted as asymmetric arbitrarily. Therefore, MWA could be used to express the equilibrium function as the rate of symmetry. In this study, the decrease of the rate of asymmetry from 36.29±4.09% to 28.17±1.72% could be an evidence of the enhanced equilibrium function targeting the subject even though subject’s asymmetry was still remained. We observed the change of MTFV after treatment that the subject showed faster velocity of her maximum trunk flexion comparing to the baseline mean of MTFV. Improved kinematics around pelvic movement in the sagittal plane could be caused by enhancement of equilibrium, or vice versa (Kwon et al., 2011). Because MTFV is one of major movement around pelvis, therefore, the subject’s improvement in balance ability was examined by faster MTFV from 61.17±8.09°/sec to 62.74±3.86°/sec. In MTEV evaluation, the same result was found that faster velocity was examined to be increased from 57.36±6.62°/sec to 62.74±3.86°/sec. In reviewing all factors to be tested for the subject in this study, the improvements of balance function were identified by enhanced WTT, MRI, MWA, MTFV, and MTEV in performing STS motion.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.