The relationship between attention deficit hyperactivity disorder and health-related physical fitness in university students
Article information
Abstract
College students with a tendency toward attention deficit/hyperactivity disorder (ADHD) tend to act impulsively because they cannot control their behavior. They display low academic achievement and insufficient social skills, and are at high risk for alcoholism and drug abuse. Although various intervention methods have been used to reduce ADHD tendency (e.g., improving physical fitness and participating in sports and exercise), there are few studies on the relationship between ADHD and health-related physical fitness. Accordingly, this study explored the relationship between ADHD symptoms in college students and physical fitness. We measured health-related physical fitness and ADHD in 86 male college students using a self-report rating scale. The results showed the following. First, a significant relationship was found between ADHD tendency and inattention/memory problems, hyperactivity/restlessness, impulsivity/emotional lability, and abdominal fat. Push-ups were associated with ADHD tendency and the inattention/memory problems, hyperactivity/restlessness, impulsivity/emotional lability, and problems with self-concept subtests. Grip strength was significantly related to inattention/memory problems. Second, risk factors for ADHD tendency significantly increased for male college students with low muscular strength and endurance relative to those with greater muscular strength and endurance. Risk factors also significantly increased for male college students with high rates of abdominal obesity.
INTRODUCTION
ADHD is a neurobiological disorder frequently observed in preschool and school-age children and has an incidence rate of 2–18% among children (Moss et al., 2007). Its prevalence rate is very high, accounting for approximately 50% of adolescent patients who visited a psychiatric clinic (Cantwell, 1996). Although ADHD is primarily a childhood disorder that used to be expected to improve with age, various longitudinal studies have now shown that it is a chronic disorder that persists into adulthood. Thus, interest in ADHD is increasing. There are cases in which 50–65% of children diagnosed with ADHD show symptoms into adulthood, and the prevalence rate of adult ADHD in the general population is estimated to be approximately 2–3% (Kim et al., 2005). In addition, approximately 25% of college students have been diagnosed with ADHD or show ADHD symptoms. However, the testing tools and countries differ from study to study, and the ADHD prevalence rate has been reported to be higher for male than for female students (Green and Rabiner, 2012). Because ADHD symptoms include low concentration, carelessness, excessive activity, and impulsivity, affected college students have poor academic performance, difficulty interacting with peers, and high rates of alcohol and drug use. In addition, because they experience repeated failure and frustration, frequent criticism, and reproach in everyday life, they often develop low self-esteem (Faraone et al., 2000). Low self-esteem and lack of sociality also cause problems in interpersonal relationships, relationships with the opposite sex, and couple and family relationships. Moreover, because the incidence rate of psychopathology (e.g., antisocial behavior and mood disorders) is high in individuals with ADHD, a therapeutic approach is needed to address emotional problems.
To date, medications, such as central nervous system stimulants (e.g., D-amphetamine or methylphenidate) and antidepressants (e.g., imipramine), are widely used as ADHD treatments. Additionally, therapeutic intervention methods, such as behavioral therapy and individual counseling, which focus on emotional problems, are applied. To overcome the limitations of medication and cognitive- and behavioral-therapy interventions, researchers have recently aimed to change ADHD behavior by using intervention variations that require physical activity e.g., exercise therapy.
When physical activity, exercise, and a wide range of movements that involve physical functions (i.e., muscular strength, endurance, and flexibility) are included in everyday life, motor skills are developed in coordination with respiration, energy production, and support of the circulatory system, muscles, and other tissues (Mikkelsson et al., 2005). This activity is useful for overcoming disabilities and making improvements. However, these physical factors can maintain function or delay function loss only when exercise and physical activity are regular and consistent (Blair et al., 1995). According to research on the effects of physical fitness on health, good physical fitness prevents cardiovascular disease and colorectal, thoracic, and various other cancers, thus contributing to the prevention of premature mortality. Physical fitness directly affects metabolic syndrome, diabetes, and hypertension and has a direct relation to human life (Ekelund et al., 1988; Kim et al., 2012; Sandvik et al., 1993). Moreover, although studies on mental health and concentration, psychological traits, anxiety, and self-esteem have all reported that regular exercise and maintaining adequate physical fitness are associated with cardiorespiratory endurance, muscular strength, and flexibility (Pontifex et al., 2012), there are few studies on the relationship between mental disability and physical fitness and especially on the relationship between ADHD and physical fitness. There is also a lack of studies exploring which physical factors affect ADHD tendency. This study examined the relationship between physical fitness and ADHD tendency in college students.
MATERIALS AND METHODS
Participants
After explaining the objectives of this study to students attending college in the Seoul-Inchon area, an ADHD self-report rating scale and health-related physical-fitness tests were conducted with students who wished to participate. The general characteristics of the 86 male college students who participated are shown in Table 1.
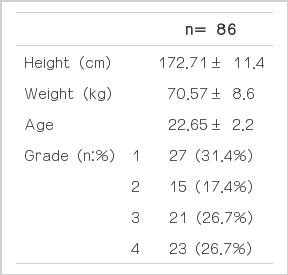
Demographics
Conners’ adult ADHD rating scale
The ADHD rating scale used in this study consisted of 4 sub-tests (inattention/memory problems, hyperactivity/restlessness, impulsivity/emotional lability, and problems with self-concept). The current study used the short version (26 questions) that Jang (2010) produced from Conners’ long version (66 questions) using the reliability of the adult ADHD rating scale as a reasonable measurement tool. A 4-point Likert-type scale was used in which the response options ranged from 0 (“not at all”) to 3 (“very often”). Internal consistency (Cronbach’s) was α=0.93 in this study.
Health-related physical-fitness tests
The 20 m PACER was used as a cardiorespiratory endurance test. Participants were asked to start at the sound of music and a buzzer and to run 20 m forward. They were then asked to wait at the other end until the next buzzer sounded, at which point they were to run in the opposite direction. A muscular strength test using grip strength measured participants’ ability to produce maximum force. After adjusting the width of a digital dynamometer (TKK, JAPAN) to fit their hands (the second knuckle of the middle finger should grip the finger stop in the proper position), participants were asked to grip the device and encouraged to pull as hard as they could. Two measurements were performed for each side, and the highest value was recorded. Muscular endurance measures how long one can continuously produce force. In this study, the physical-fitness test items of sit-ups and push-ups were conducted to test muscular endurance. For the sit-ups, participants were asked to lie on a mat with both knees drawn up and their feet flat on the ground. With both hands placed on their thighs, they were asked to lift the upper body so both hands touched their knees. Participants were asked to do one sit-up every 3 sec in time with a beep. The number of sit-ups completed until the participant was unable to complete 2 consecutive sit-ups was recorded. For the push-ups, the participants were asked to keep their legs straight, spread their arms to the width of their shoulders, and stretch out from head to shoulder through the back, waist, hips, and knees. They were asked to set their elbows on the floor at a 90° angle and to maintain that stance as the “ready position.” Push-ups were performed at 2-sec intervals, and the number of push-ups participants were able to complete was recorded. Sit-and-reach measures the flexibility of the waist. This measurement was performed by asking the participants to stretch both legs out in front of them with the soles of their bare feet flat against the flexometer (the “sit-and-reach box”) and to slowly reach forward with the middle fingers of both hands pushing on the sit-and-reach box. To ensure that the participants’ knees were not bent, a tester pressed on their knees. The sit-and-reach test was conducted with a starting value of −20 cm. Abdominal fat percentage was measured using the InBody 720 body composition test.
Data analysis
All data were analyzed using SPSS/IBM 21. The mean and standard deviation of each item were calculated in accordance with the study objective. A correlation coefficient was calculated to explore the correlation between physical factors and ADHD items. By dividing participants into 3 groups (tertiles: low 33.3%, mid 33.3%, high 33.3%) according to level of physical fitness and using ANOVA, mean values of each group were compared. Post-hoc tests were conducted using the Scheffé method. The statistical significance level in all analyses was set at P<0.05.
RESULTS
Correlation between ADHD and health-related physical fitness
Analysis of the correlation between participants’ ADHD rating-scale score and physical fitness showed that abdominal fat percentage was related to impulsivity/emotional lability, hyperactivity/restlessness, irritability, and inattention/memory problems (Table 2). It also showed that push-ups, which were used to measure muscular endurance, were associated with the ADHD problems with self-concept, impulsivity/emotional lability, hyperactivity/restlessness, and inattention/memory problems subtests. In addition, grip strength was associated with the inattention/memory problems subtest (Table 3).

Participates’ ADHD and health-related physical fitness level

Correlation between ADHD and related-health physical fitness
Relationship between ADHD and health-related physical fitness
The correlations between participants’ physical-fitness tests and ADHD tendencies and the differences in ADHD tendencies are presented in Tables 4–6 according to level of physical fitness (low, mid, high). It was found that participants with high abdominal obesity had a higher propensity to show ADHD, inattention/memory problems, and hyperactivity/restlessness than those with low abdominal obesity (Table 4). It was also found that those with low muscular strength (grip strength) had a higher propensity to experience ADHD and inattention/memory problems than those with greater muscular strength (Table 5), and those with low muscular endurance (push-ups) were more likely to show ADHD, inattention/memory problems, and impulsiveness/emotional lability than those with high muscular endurance (Table 6).

Difference ADHD according to abdominal fat %
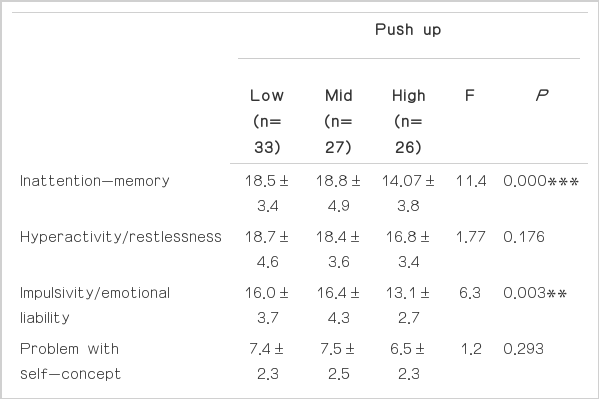
Difference ADHD according to push up

Difference ADHD according to grip strength
DISCUSSION
This study confirmed a close relationship between participants’ muscular strength and endurance, abdominal obesity, and flexibility and their risk factors for ADHD. In addition, this study, which targeted college students, found that risk factors for ADHD significantly increased for male college students with low levels of physical fitness compared to those with high levels. That is, as the rate of abdominal obesity increased, risk factors for ADHD tendency significantly increased, and risk factors for ADHD tendency increased for male college students with low muscular strength and endurance compared to those with high muscular strength and endurance. ADHD refers to a situation in which problems are caused by a lack of ability to properly control oneself.
A genetic problem with the brain’s control function is a cause of ADHD. In other words, ADHD is a dysfunction caused by a problem with the connection pathway linking the frontal lobe and basal ganglia, which are brain areas that control improper behavior. There is an imbalance in the level of the neurotransmitters, the chemical substances that deliver signals to these sections (Geen and Rabiner, 2012; Moss et al., 2007). Muscle, as flesh that produces force, relates directly to motor ability. The contraction and relaxation of muscles causes movement in all organs of the body. Furthermore, when muscles move, nerves, ligaments, and tendons all have a function in controlling the body to prevent injuries. In particular, the brain functions as the command center that orders muscles to move slowly or rapidly by delivering information through nerves. When muscles are in motion, an appropriate level of excitatory neurotransmitters is secreted in the brain, enabling the body to move. If the brain’s excitatory neurotransmitters are depleted or excessively secreted, the muscles will move involuntarily (So and Oh, 2008).
The results of this study showed that muscular endurance (as measured by push-ups) is closely related to ADHD tendency. Examination of the methods for completing push-ups indicates that it is a motion requiring force and coordination of the arms and body as a whole. Because push-ups measure how long one can perform in a state in which force and coordination are in harmony, the current results support the notion that it is a physiological mechanism in which an appropriate level of neurotransmitters is secreted when one is in motion. Obesity leads to physiological aspects of disease and affects risk factors for ADHD.
According to previous studies on the physiological aspects of obesity, obesity affects metabolic syndromes, hypertension, diabetes, and mental health (Converse et al., 2014; Kim et al., 2012; Moon et al., 2012; Pontifex et al., 2012). It has been reported that students with mental disorders or attention deficit disorder have a high rate of playing games on the internet or using cell phones rather than engaging in regular exercise or playing sports (So and Oh, 2008). Thus, they spend a lot of time sitting down, which is expected to affect abdominal obesity. As shown in the results of this study, there was a relationship between abdominal obesity and ADHD tendency. This implies that male college students with a high ADHD tendency will likely have low levels of physical activity. Accordingly, a study on the relationship between amount of physical activity and ADHD tendency should be conducted in the future. Furthermore, if an exercise program that improves muscular strength and endurance (i.e., one that allows continuous exercise by controlling muscles and nerves) were developed and applied, it would contribute to a reduction in ADHD tendency in male college students.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.