Isokinetic dynamometer evaluation of the effects of early thigh diameter difference on thigh muscle strength in patients undergoing anterior cruciate ligament reconstruction with hamstring tendon graft
Article information
Abstract
After anterior cruciate ligament (ACL) reconstruction, which muscle groups are more affected from frequently developing thigh muscle atrophy is a matter of debate. We evaluate the effect of thigh circumference difference between patients’ knees who were administered the ACL reconstruction with hamstring tendon autograft and intact knees, on torque between the hamstring and quadriceps muscles. Fifty-five patients at least 6 months follow-up period available were included in our study. Power measurements of quadriceps and hamstring muscle groups in patients’ extremities were done by using isokinetic dynamometer. The maximum torque values at 60°/sec, 240°/sec in frequency, positions of flexion and extension were determined. In accordance with our findings it is still possible to encounter the thigh atrophy in average 28 months after ACL reconstruction surgery even under physical rehabilitation programs and appropriate follow-up. It is inevitable for the clinician to consider these changes in diagnosis and rehabilitation stages. It can’t be ignored that muscle weakness mechanisms developing in the thigh circumference vary according to the thigh muscle group and knee flexors play an important role in thigh atrophy when determining an appropriate rehabilitation program after reconstruction application.
INTRODUCTION
Anterior cruciate ligament (ACL) has a primary role in the limitation of anterior translation of the tibia as regards to the femur. Hamstrings play a major role in protecting the ACL. They are also important for the compensation of stability in the ACL in the knee lesions and patients with ACL. The hamstring muscle weakness and hamstrings’ weak relationship with the quadriceps are risk factors for ACL injuries. Various surgical methods are defined for in the treatment of anterior cruciate ligament. One of the most commonly used treatments is the method in which knee flexor tendons are used as autograft. As shown in previous studies, after using this method reconstructed knee recovered up to the 90% of flexion muscle strength of counter knee (Harter et al., 1990; Lipscomb et al., 1982; Simonian et al., 1997). It is also shown in previous studies that semitendinosus which is also used as ACL graft has regeneration potential from more proximal and with similar morphology (Eriksson et al., 2001; Ferretti et al., 2002; Hioki et al., 2003; Nakamae et al., 2005; Simonian et al., 1997; Williams et al., 2004). Although there is a development of regeneration close to normal morphology; knee flexors’ abnormalities in neurological function can be a barrier to motor units’ function by preventing their healing. Hamstring weakness after ACL rupture is associated with weakness in knee function. However, morphological factors such as muscle atrophy in these patients is not the only factor that determines the maximum power; in previous studies, it is shown that despite the absence of morphological abnormalities the afferent feedback deficiency from ACL may interfere with the activation of gamma motor unit of the muscles around the knee (Konishi et al., 2002a; 2002b; 2003; 2007a; 2007b).
Therefore, even if the knee flexor tendon regeneration is morphologically normal and that motor unit complex may prevent the function of the knee flexors by causing neurologic abnormalities. Therefore, while comparing knee flexor muscle strength of patients who underwent ACL reconstruction with normal uninjured knee, muscle weakness due to the possibility of neurologic abnormalities can not be ignored.
After ACL reconstruction, which muscle groups are more affected from frequently developing thigh muscle atrophy is a matter of debate. Muscle strength tests are used to evaluate recovery of ACL after treatment and the effectiveness of treatment. According to the study carried out, after ACL reconstruction using hamstring tendon grafts, weakness in the knee flexor muscle strength can be observed up to 24 months. In addition, previous studies showed that in patients who underwent ACL reconstruction quadriceps muscle torque per unit volume is significantly lower compared the intact knee (Konishi et al., 2007b).
In our study, we aimed to evaluate the effect of thigh circumference difference between patients’ knees who were administered the ACL reconstruction with hamstring tendon autograft and intact knees, on torque between the hamstring and quadriceps muscles. As is known, development of muscle weakness in quadriceps after ACL lesions caused by neurological dysfunction was shown to be a natural consequence. In our study, we planned to evaluate the effect of thigh circumference difference between operated extremity and intact extremity on knee flexors’muscle strength.
MATERIALS AND METHODS
Fifty-five patients (54 males, 1 female, mean age 28.15±6.47) who underwent ACL reconstruction in our clinic and with at least 6 months follow-up period available were included in our study. While choosing the patients, not having any disease nor interventions previously on intact knees has taken into account. Patients who have symptoms and signs such as discharge, inflammation, instability, locking, limitation of motion, anxiety while exercising were removed from the study. All operations were applied in teaching and research hospital by the same surgeon. The condition that autogenous hamstring tendon graft usage in ACL reconstruction was searched for the patients. In all patients, same postoperative rehabilitation program which is indicated below was applied with attention. For the first week walking with a full load, 0°–90° of passive knee extension, bringing the active flexion, quadriceps and hamstring muscle training, heel shift, straight leg rise; between 1–2 weeks, hamstring training in the prone position, asideleg lift, walkingin the water if a swimming pool exist; between 2–3 weeks, terminal extension and hamstring stretch studies with weight; 3–4 weeks, if knee flexion has reached to 90° the pedals ergonometric work, walking back in the pool (if possible), doing full daily activities; 6–12 weeks, rising at finger tips and starting to closed kinetic chain exercises, preparations for the transition to the sport aiming to increase strength, durability and propsiosepsiyo; In the 3rd month, cycling, running and scissoring in water; in the 4th month, in addition to weight training activities beginning to proprioceptive and on the stairs activities, doing straight running; in 6–8 months beginning to sport-specific movements, ensuring to return to contact sports were taken into account.
Each patient was laid in the supine position, knees at full extension and relaxed position prior to measurement of the circumference of the thigh muscles. Both thigh circumference were measured and recorded from 15 cm proximal to the upper limit of the patella for measuring. The determined length difference between there constructed knee and the intact knee was taken.
Power measurements of quadriceps and hamstring muscle groups in patients’ extremities who underwent operation and who did not in were done by using Cybex II dynamometer (Humac). During the measurements the maximum torque (peak torque) values at 60°/sec, 240°/sec infrequency, positions of flexion and extension were determined. Measured values between the operated and non-operated extremities have been compared to each other. The application of standard equipment, data collection and heating procedures were performed before the measurement. Patients were told to continue their usual daily activities not to do tiring activities in the day before the test. On the test day before the beginning of measurements patients were carried out a 5-minute warm-up exercises on a stationary bike. Patients’ pelvis were stabilized with the help of a belt, thighs were supported with pillows, ankle cuff was placed directly on top of malleolar. Patients’ forearms were positioned so that the rotational axis of the forearms were aligned with rotational axis of knees.
During the test the range of motion was adjusted to be 0° extension and 90° flexion. In order to get support patients were allowed to hold seats on the sidebar during the test. Before starting the recording of the data patients did three times sample repetition at both angle rates. Concentric exercise were carried out for 5 times in maximal flexion and extension to patients after one minute rest. First, 60°/sec speed after a minute rest the test was continued with 240°/sec speed. Patients were encouraged verbally to show maximum effort. Several patients developed thigh pain during measurements and measurements were repeated after the test was terminated.
RESULTS
Number Cruncher Statistical System (NCSS) 2007 and Power Analysis and Sample Size (PASS) 2008 Statistical Software (Utah, USA) were used for statistical analysis. Besides descriptive statistical methods (mean, standard deviation, median, frequency, rate, minimum, maximum) for qualitative comparison of data Pearson’s chi-square test, Fisher-Freeman-Halton test, Fisher’s exact test, and Yates Continuity Correction test (Yates adjusted Chi-square) were used for the evaluation of data. Spearman’s correlation analysis was used to assess the relationships between parameters. Significance at P<0.01 and P<0.05 levels were evaluated.
Age identifier values and follow-up periods of patients are shown in Table 1. Thigh circumference of intact extremity and operated extremity of patients are shown in Table 2. Peak torque of the mean extensor and flexor muscle strength and percentage values relative to each other, are shown in Tables 3, 4, and 5.

The distribution of descriptive characteristics

Evaluation of patients thigh diameter difference (n= 55)

Distribution of cybex extension and flexion measurement of the patients
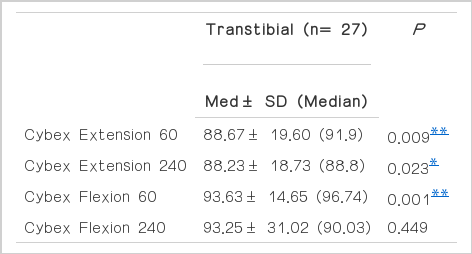
Evaluation of cybex extension and flexion measurement of the patients

Distribution of cybex extension and flexion measurement of the patients
Statistically significant relationship was observed at the level of 66.0% percent between the thigh diameter difference and Cybex Extension 60 of patients in negative direction (while the thigh diameter difference increasing the Cybex Extension 60 percent decreasing) (r: −0,660; P=0.001; P<0.01).
Statistically significant relationship was observed at the level of 55.0% percent between the thigh diameter difference and Cybex Extension 240 of patients in negative direction (while the thigh diameter difference increasing the Cybex Extension 240 percent decreasing) (r: −0,550; P=0.005; P<0.01) (Fig. 1).

Cybex extension.
Statistically significant relationship was observed at the level of 55.0% percent between the thigh diameter difference and Cybex Flexion 60 of patients in negative direction (while the thigh diameter difference increasing the Cybex Flexion 60 percent decreasing) (r: −0,555; P=0.002; P<0.01).
It was observed a relation between the thigh diameter difference and Cybex Flexion 240 of patients in negative direction (while the thigh diameter difference increasing the Cybex Flexion 240 percent decreasing) at the level of 28.1% percent and this situation was found to be statistically significant (r: −0,281; P=0.079; P>0.05) (Fig. 2).
Cybex flexion.
DISCUSSION
After our study, in accordance with our findings it is still possible to encounter the thigh atrophy in average 28 months after ACL reconstruction surgery even under physical rehabilitation programs and appropriate follow-up. In line with earlier studies, quadriceps muscle mass is often seen as responsible for the present thigh atrophy, however negative effects of the hamstring muscle group on muscle atrophy which is determined with manual thigh circumference measurements are undeniable. As shown in previous studies, in patients with ACL lesions the development of neurological dysfunction is not available in the knee flexors comparing with quadriceps muscle group.
Comparative studies which was done in patients with ACL lesion and in patients without any knee problems showed that there was no significant difference between the speed of flexion and torque per unit volume of the knee flexor muscle. Despite this, in the same study it was found that isokinetic torque that occurred in the knee with ACL lesions at 60°/sec was less than robust knee (Konishi et al., 2012). In addition, it is shown that the ACL reconstruction with hamstring tendon is not effective on muscle torque power of knee flexors and flexion speed of these muscles by showing that detection of changes in the robust knee is the same. In the light of these data, it might lead to think that ACL lesions does not cause neurological dysfunction in the knee flexors. In another study there was a comparison between patients who were administered to the ACL reconstruction and patients who did not have any knee problem, it has been identified that muscle torque power on per unit volume of the quadriceps was significantly lower in the patients who were administered to reconstruction. In addition, quadriceps weakness is associated with the neurologic dysfunction that is developed after ACL reconstruction has been shown by other researchers (Hart et al., 2010; Rice et al., 2009; Snyder-Mackler et al., 1994; Urbach et al., 1999; 2002). It has been shown that muscle weakness in the quadriceps that is induced by the ACL lesions is a natural result linked to the development of neurological dysfunction.
In our study we have showed the loss of torque power of thigh atrophy on quadriceps at the 60°/sec, 240°/sec frequency even in the patients who have an appropriate rehabilitation program after ACL reconstruction and under going follow-up process. Although, it has been shown in previous studies that ACL lesion development in the thigh did not lead to neurological dysfunction on hamstring; in our measurements, it has been determined statistically that atrophy developed in the thigh is effective on the hamstrings muscle torque power at least as it is on quadriceps, especially 60°/sec frequency. It could not be shown that this weakness is correlated to thigh atrophy as well as quadriceps at 240°/sec flexion frequency.
In addition, treatment of quadriceps weakness developing after ACL injuries is difficult. These difficulties are likely to be related to neurological dysfunction occurred in the quadriceps muscles. Due to different muscle weakness mechanisms which are developing according to the morphological structure and muscle properties, it is inevitable for the clinician to consider these changes in diagnosis and rehabilitation stages. The point that we want to emphasize in our study is; it can’t be ignored that muscle weakness mechanisms developing in the thigh circumference vary according to the thigh muscle group and knee flexors play an important role in thigh atrophy when determining an appropriate rehabilitation program after anterior cruciate ligament reconstruction application.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.