The relationship between the behavior problems and motor skills of students with intellectual disability
Article information
Abstract
The purpose of this study was to determine the relationship between the motor skills and the behavior problems of students with intellectual disabilities. The study participants were 117 students with intellectual disabilities who were between 7 and 25 years old (male, n=79; female, n=38) and attending special education schools in South Korea. Motor skill abilities were assessed by using the second version of the Bruininks-Oseretsky test of motor proficiency, which includes subtests in fine motor control, manual coordination, body coordination, strength, and agility. Data were analyzed with SPSS IBM 21 by using correlation and regression analyses, and the significance level was set at P<0.05. The results showed that fine motor precision and integration had a statistically significant influence on aggressive behavior. Manual dexterity showed a statistically significant influence on somatic complaint and anxiety/depression, and bilateral coordination had a statistically significant influence on social problems, attention problem, and aggressive behavior. Our results showed that balance had a statistically significant influence on social problems and aggressive behavior, and speed and agility had a statistically significant influence on social problems and aggressive behavior. Upper limb coordination and strength had a statistically significant influence on social problems.
INTRODUCTION
The prevalence of intellectual disability (ID), although it differs by age, is known to be approximately 1% of the total population. Meanwhile, the prevalence of severe ID is reported to be 0.6% (American Psychiatric Association, 2013). In South Korea, the population with a registered ID, including autism, consisted of 210,855 people in 2015, representing 4% of the total population, showing an increasing trend (Korean Ministry of Health and Welfare, 2016).
Children and students with intellectual disabilities are characterized by limited cognitive function, including severe deficits or limitations in individual skills in several domains as follows: cognitive, language, motor psychosocial, and specific activities of daily living (Vandorpe et al., 2012; Westendrop et al., 2011). These characteristics mean that students with ID show more problematic behaviors than typical students. These include a diverse range of problematic behaviors such as attention deficit, elopement, self-harm, aggression, feeding behavior, stereotyped behavior, attachment behavior, disruptive behavior, and impulsive behavior. These problematic behaviors deprive individuals of opportunities to participate in learning and daily living. Their impact on adaptation to relationships with friends, school education, and social life can not only cause great despair in school education but also lead to long-term social maladaptation that continues to exert a strong negative effect on employment after graduation (Park, 2004). Therefore, there can be no doubt about the massive importance of interventions for problematic behaviors in students with ID. In a meta-analysis of interventions for problematic behaviors in individuals with ID, Kim (2014) found that most interventions came from research related to special education and therefore highlighted the need for multifaceted intervention research.
In the field of physical education, various exercise-based methods are being suggested as interventions for problematic behaviors in individuals with ID. Regular physical activity and exercise help to increase adaptation and emotional stability by relieving psychological tension, anxiety, and fatigue (Jeoung, 2014; Park and Kim, 2012).
Numerous studies are being conducted based on these principles. Although studies have shown no positive effect, depending on the exercise method, or no improvement in problematic behaviors, most of these studies have shown positive effects of exercise (Choi and Roh, 2011; Jeoung, 2014; Lee and Han, 2015; Park, 2004).
Although exercise-based interventions that use a behavioral corrective or psychotherapeutic approach have been presented (Milne et al., 2016; O’Beeirne et al., 1996; Park, 2004), the application of diverse exercise methods is limited because individuals with ID have reduced capacity for physical exercise when compared with typical individuals. Opinions are contradicting regarding which types of exercise are effective at improving problematic behaviors. However, most of the previous studies have emphasized the importance of exercise development in students with ID and that exercise development is reported to have close association with cognitive and emotional development (Harris, 1981; Harvey et al., 2009).
Choi and Roh, (2011) emphasized the relationships of cognitive function and adaptive behavior in individuals with ID with the development and motor skills of the large muscles, while also highlighting the need for exercise to develop coordination of the large muscles and hand muscles. Oh et al. (1991) categorized problematic behaviors of children and youths into internalized and externalized problems, determined the causes of emotional and behavioral problems, and made predictions about the process of development (Srour and Shevell, 2014; Stodden et al., 2008). In terms of emotional and behavioral problems, children and youths with ID show problematic behaviors related to depression, anxiety, a sense of inferiority, aggression, thought problems, social immaturity, and physical symptoms (Kim, 2014; Shevell et al., 2003). These problematic behaviors are considered to reflect issues with cognitive function and adaptive behavior. Thus, although there are studies that are suggestive of a relationship of large muscle development with cognitive function and adaptive behavior in children with ID, research that investigates the direct relationship between problematic behaviors and the development of motor skills is lacking. Moreover, we anticipate that studying the effects of delayed motor development on problematic behaviors and the associations with related variables would not only provide basic data to help understand motor skill development and characteristics in children of school age but also provide significant information for the development of exercise programs to reduce problematic behaviors. Therefore, the aim of this study was to ascertain the level of motor skill development in students with ID, to identify the relationships with and the impact on problematic behaviors, and to investigate the major related variables.
MATERIALS AND METHODS
Participants
The participants in this study, who were residents of I city, included 117 students with intellectual disabilities between the ages of 8 and 21 years (male, n=79; female, n=38) who were attending special education schools in South Korea. Participant demographics are shown in Table 1.
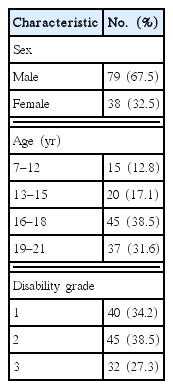
General characteristics (n=117)
Measurement
The Bruininks-Oseretsky Test of Motor Proficiency, Second Edition (BOTMP-2), is a normative referenced standards motor assessment test available in a complete form with 53 items (Bruininks and Bruininks, 2005). It is suitable for use in children aged 4 to 21 years. This version is categorized into four composite motor domains. Fine motor control includes fine motor precision (41 points) and fine motor integration (40 points). Manual coordination includes manual dexterity (45 points) and upper limb coordination (39 points). Body coordination includes bilateral coordination (24 points) and balance (37 points). Strength and agility includes running speed and agility (52 points) and strength (42 points). We performed an assessment by using the BOTMP-2. Three researchers rated each participant on the BOTMP-2 and subtest items, and average scores were calculated.
Child Behavior Checklist
This study surveyed children aged 4–17 years by parental report, using the Korean version of the Child Behavior Checklist (K-CBCL) to evaluate problematic behaviors. The K-CBCL was developed by Oh et al. (1997) based on the United States CBCL and has been standardized for Korean children. The K-CBCL is divided into social ability and problematic behavior syndrome scales, but the present study only used the problematic behavior syndrome scale. The problematic behavior syndrome scale consists of 8 subscales that measure withdrawal, somatic complaint, anxiety/depression, social immaturity, thought problems, attention problems, rule breaking, and aggression. The problematic behavior syndrome scale of the K-CBCL contains 119 items, and each item is rated on a 3-point Likert scale of 0 points (none), 1 point (behavior is infrequent or mild), and 2 points (behavior is frequent or severe). Each subscale in the problematic behavior syndrome scale is evaluated by summing the scores for each item in the scale. As the whole problematic behavior syndrome scale consists of 117 items, the range of possible scores is 0–234. The score can be converted into a standardized score (T score) based on the standard criteria. For the internalized problem, externalized problem scale, and whole problematic behavior scales, a T score of ≥63 is considered to be in the clinical range. Meanwhile, for each of the 10 subscales, T scores of ≥70 are considered to be in the clinical range. The reliability of the CBCL has been assessed with a Cronbach α of 0.65–0.85.
Data analysis
Data were analyzed with IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA). Descriptive statistics were used according to the study objectives, and a bivariate correlation analysis was performed to examine the relationship between motor skills and cognitive function. A line regression was performed on motor skill subdomains that showed a significant correlation to analyze their effects on subdomains of cognitive function. The level of significance was set at P<0.05.
RESULTS
Table 2 shows the results of the analysis of the correlations between the problematic behaviors and the motor skills of students with ID. Among the subdomains of problematic behaviors, aggressive behavior was associated with the fine motor subdomain of the BOTMP-2, which was used to measure motor skills, and fine motor integration and aggressive behavior showed correlation. Manual dexterity correlated with the somatic complaint and anxiety/depression subdomains. Social problems correlated with bilateral coordination, balance, speed and agility, upper limb coordination, and strength. Attention problems were correlated with bilateral coordination. Table 3 shows the results of analysis of the effects of subdomains that showed a significant correlation.

Correlation between the behavior problems and the motor skills of the students with intellectual disabilities

Results of the regression analysis of the behavior problems and motor skills of the students with intellectual disabilities
Table 3 shows that the anxiety and depression score is predicted to increase by 0.16 for every 1 point increase in the score of the motor skill manual dexterity subdomains. The coefficient of determination that explains this change is R2=0.03. The social problem score would also predictably decrease by −0.26 (R2=0.03) as the bilateral coordination score increases by 1, and would decrease by −0.21 (R2=0.03) as the balance score increases by 1. The social problem score decreases by −0.28 (R2=0.07) as the speed and agility score increases by 1, decreases by −0.20 (R2=0.03) as the upper limb coordination score increases by 1, and decreases by −0.29 (R2=0.08) as the strength score increases by 1. The attention problem score is predicted to decrease by −0.22 (R2=0.04) as the bilateral coordination score increases. The aggressive behavior score is predicted to decrease by 0.21 (R2=0.03) and decrease by −0.18 (R2=0.02) as the fine motor score increases by 1. The aggressive behavior score decreases by −0.18 (R2=0.02) as the fine motor integration score increases by 1, decreases by 0.24 (R2= 0.04) as the bilateral coordination score increases by 1, decreases by −1.95 (R2=0.03) as the balance score increases by 1, and decreases by −0.15 (R2=0.01) as the speed and agility score increases by 1. These changes are statistically significant.
DISCUSSION
This study investigated the effects of motor skill development on behavioral problems in students with ID. We found that among subdomains of problematic behaviors, social problems were associated with the motor skill developmental subdomains of bilateral coordination, balance, speed and agility, upper limb coordination, and strength. These results demonstrate that increased coordination and gross motor development help to improve social problems. A study by Choi and Roh (2011) also showed the same results, where gross motor development affected sociability as a subdomain of adaptive behavior development. The study by Choi and Roh (2011) only measured four items from the BOTMP (speed, balance, coordination, and strength) to analyze their relationships with adaptive behaviors. Unfortunately, they did not also study the relationships with fine motor integration and manual dexterity in the fine motor domain. Nevertheless, their results were consistent with our results for the variables that were investigated.
As shown by the results of our study, aggressive behavior correlated with the fine motor domain, fine motor integration, bilateral coordination, balance, and speed and agility. In other words, fine motor control can be considered necessary to improve aggressive behavior (Higgins and George, 2006; Vrijmoeth et al., 2012). The parts of the brain that control aggression are directly connected to the brainstem nuclei, the amygdala, and the frontal lobe. The hypothalamus expresses receptors that help determine the extent of aggression, through interactions between neurotransmitters such as serotonin and vasopressin (Choo et al., 2008). The roles of the brainstem include primitive functions such as consciousness, breathing, and balance. In particular, it is responsible for controlling the functions of the four limbs. The functions of the frontal lobe include motor and intellectual functions. Specifically, it is responsible for establishing and executing plans. Based on this evidence, the development of motor skills can be considered necessary for controlling aggression. This study also demonstrates a relationship between attention problem and bilateral coordination. The part of the brain that controls attention is the frontal lobe, which also acts in thinking and behavioral control. More precisely, it plays a key role in judgment, emotional control, control of attention, planning, and memory (Ferris et al., 1996). The movements used to measure bilateral coordination include touching the nose with the index fingers with eyes closed, jumping jacks, jumping in place with the leg and arm on the same side synchronized, jumping in place with the legs and arms on the opposite sides synchronized, pivoting thumbs and index fingers, and tapping feet and fingers (same side and opposite sides synchronized). These movements are only possible with integrated control in the frontal lobe and can be considered to affect attention for this reason (Choo et al., 2008).
Finally, the anxiety/depression subdomain was shown to be correlated with manual dexterity. Brain regions known to be related to anxiety include the amygdala, prefrontal cortex, hippocampus, and basal ganglia. The basal ganglia are involved in movement and motor function, while the amygdala receives information about warnings and rapidly sends signals to the muscles, autonomic nervous system, and pituitary gland. Brain regions related to depression also include the prefrontal cortex, anterior cingulate cortex, amygdala, and hypothalamus (Choo et al., 2008; Potegal et al., 1996). Therefore, improving problematic behaviors can form the basis for developing motor skills in students with ID and can have an important influence on the formation of balanced motor skills during childhood. Based on the results of our study, we can assume a relationship between the functions of the brain that cause problematic behaviors and the areas of the brain that control motor function. In the future, broader research will be required to improve problematic behaviors, such as studies that investigate changes in brain tissue in relation to the level of motor function development.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.