Changes in gait kinematics and muscle activity in stroke patients wearing various arm slings
Article information
Abstract
Stroke patients often use various arm slings, but the effects of different slings on the joint kinematics and muscle activity of the arm in the gait have not been investigated. The effects of joint kinematics and muscle activity in the gait were investigated to provide suggestions for gait training for stroke patients. In all, 10 chronic stroke patients were voluntarily recruited. An eight-camera three-dimensional motion analysis system was used to measure joint kinematics while walking; simultaneously, electromyography data were collected for the anterior and posterior deltoids and latissimus dorsi. The amplitude of pelvic rotation on the less-affected side differed significantly among the different arm slings (P<0.05). Changes in the knee kinematics of the less-affected side also differed significantly (P<0.05), while there were no significant differences in the muscle activity of the affected arm. In stroke patients, an extended arm sling is more useful than no sling or a flexed arm sling in terms of the amplitude of the rotation of the less-affected pelvic side in the stance phase while walking. The less-affected knee joint is flexed more without a sling than with any sling. All arm slings support the extension of the contralateral knee.
INTRODUCTION
Stroke is a major cause of morbidity worldwide. Approximately 800,000 patients have strokes annually (Lloyd-Jones et al., 2010). Patients with stroke have disabilities that result from paralysis, and most complain of difficulty walking (Jørgensen et al., 1995). Bovonsunthonchai et al. (2012) showed that the affected upper extremity is important for improving the performance and coordination of gait in stroke patients. In addition, the movement of the upper extremity improves the range of motion at the ankle as well as trunk stability (Stephenson et al., 2010).
Stroke patients often develop a subluxation of the shoulder on the affected side, because they can no longer support the weight of their own arm due to paralysis (Griffin et al., 1986). Consequently, arm slings are often necessary. Stroke patients often use a hemisling. Faghri et al. (1994) stated that use of a hemisling induced flexion synergy patterns of the upper trunk and delayed functional activity. However, few studies have examined how different arm slings, including a hemisling, affect the gait patterns of stroke patients. Reported studies have examined the hemisling in terms of the gait patterns (Yavuzer and Ergin, 2002), balance (Acar and Karatas, 2010), and energy consumption (Han et al., 2011) of stroke patients.
There are various types of arm sling, such as the flexed sling (a single-strap hemisling), extended sling (Bobath sling, Rolyan sling), GivMohr sling (Dieruf et al., 2005), and elastic arm sling (Hwang and An, 2015). The sling supports some of the weight of the arm and simultaneously limits the motion of the upper extremities. Pontzer et al. (2009) suggested that the arms serve as passive mass dampers to decrease the rotation of the torso and head. Lieberman et al. (2007, 2008) also held that the arms serve as passive dampers to minimise vertical motion. The trunk and shoulders act as elastic linkages between the pelvis, shoulder girdle, and arms (Pontzer et al., 2009).
Some studies have examined the activities of the arm muscle during walking (Lieberman et al., 2007; Prentice et al., 2001), while other studies have found that most of the arm swing is passive, while a small torque may actively occur in shoulder rotation (Jackson et al., 1978; Kubo et al., 2004). The muscle activity of the upper extremities is still the subject of debate (Collins et al., 2009; Kubo et al., 2004; Kuhtz-Buschbeck and Jing, 2012). However, the restrictive effects and support provided by various arm slings could have different effects on the muscle activities of the affected arm in stroke patients.
Therefore, we investigated how the muscle activities of the affected arm and kinematic data taken during walking are influenced by flexion-type (hemisling), extension-type (Rolyan sling), and elastic arm slings under elastic tension. We discuss which arm should be used for clinical gait training.
MATERIALS AND METHODS
Study participants
In all, 10 patients who had experienced a stroke (male, 5; female, 5) volunteered to participate in this study. Basic demographic information was obtained, including diagnosis, affected side, and postonset changes. The characteristics of the participants are summarized in Table 1. Inclusion criteria were as follows: diagnosis of stroke due to infarction or haemorrhage, score over 21 on the Mini-Mental Status Examination and ability to walk independently or with a cane. Exclusion criteria were as follows: medical problems that affect the gait pattern other than the neurological lesion, bilateral affected limbs or a premorbid or current orthopaedic problem related to the feet. The study was approved by the institutional review board at Hoseo University. All participants understood the procedures used in this study and gave written informed consent before participation.
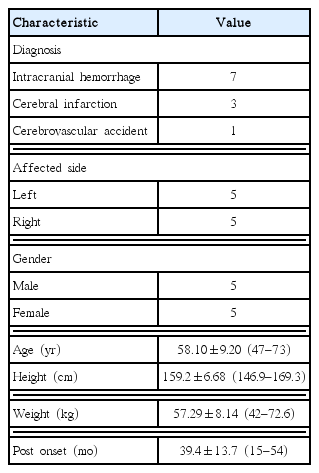
Characteristics of the participants
Gait kinematics
An eight-camera three-dimensional motion analysis system (Vicon, Fareham, UK) was used to evaluate the transverse and sagittal kinematics of both lower extremities (pelvis, hips, knees, and ankles) at a sampling rate of 100 Hz (Yoon et al., 2016). To evaluate the kinematics of the lower extremities, 16 markers were attached to the subjects bilaterally, as follows: the anterior and posterior superior iliac spines, the lower lateral 1/4 surface of the thigh, the lateral epicondyle of the knee, the lateral malleolus, the lower 1/3 of the shank, the second metatarsal head, and the posterior calcaneus. To minimise error, one experienced researcher attached all of the markers (Yoon et al., 2016).
Muscle activity
The activities of the anterior deltoid, posterior deltoid, and latissimus dorsi muscles were recorded using a Delsys Trigno Wireless EMG system (Delsys, Natick, MA, USA), which was synchronised with a Vicon Motion System. To compare muscle activity and other data, subjects performed a maximal normalisation contraction of each muscle on the affected side 3 times and obtained acceptable signals. The surface electrode placement for the three muscles was as follows: anterior deltoid, within an elongated oval below the lateral end of the clavicle; posterior deltoid, two fingerbreadths behind the acromion; and latissimus dorsi, below the inferior angle of the scapula (Perotto et al., 2011; Xu et al., 2014). Before the electrodes were applied, the skin was shaved and wiped with a cotton swab soaked in alcohol.
Procedures
Before the procedure, the investigator demonstrated a walk in front of the subjects. A seat was available for rest before and after each test. The activities of the anterior and posterior deltoid and latissimus dorsi muscles of all subjects were monitored by surface electromyography (EMG) while walking. The subjects prepared for their walk while standing, and performed the walk under four conditions in random order: no sling, a flexed sling (a hemisling), an extended arm sling (Rolyan sling), and an elastic arm sling (Fig. 1). All subjects performed each test twice and were allowed 2 min between tests. The elastic arm sling designed by Hwang and An (2015) was employed, using the green elastic tension band, as in their study. One experienced researcher adjusted the elastic arm sling to control the tension so that it was comfortable for the subjects.

The conditions of the various arm slings: (A) none, (B) a flexed type, (C) an extended type, and (D) an elastic type.
Data analysis
Motion data were captured and the marker trajectories were post-processed using Nexus 1.7 software (Vicon, Fareham, UK). The kinematics of the pelvis and hip were defined as rotation in the transverse plane in the stance phase. The amplitude of the pelvic and hip motion was calculated as the maximum value minus the minimum value. The ranges of angles of the hips, knees, and ankles were determined for the affected and non-affected sides in the stance phase. EMG signals were sampled at 2,000 Hz and filtered at 20–450 Hz. The root mean square values of the signals were calculated. For normalisation, EMG data were reported as a percentage of maximal voluntary contraction.
Statistical analysis
Friedman test (SPSS ver. 20.0, SPSS Inc., Chicago, IL, USA) was used to assess the effects of wearing the different arm slings on the kinematic data during the gait and muscle activities of the affected arm. Post hoc analyses were conducted using the Wilcoxon matched-pairs signed-rank test. The level of significance was set at P<0.05.
RESULTS
The results are given as the degrees of pelvic rotation and hip, knee, and ankle sagittal angle using the different arm slings. In the stance phase, the amplitude of pelvic rotation significantly (P<0.05) differed among the slings on the less-affected side but not on the affected side (Table 2). Specifically, the rotation significantly differed between the extended arm sling and both the flexed arm sling and no sling (P<0.05) (Fig. 2). There were no differences in the angles of the hip, knee, and ankle on the two sides, but the minimum knee angle on the less-affected side significantly differed between all slings and having no sling (Table 2, Fig. 3).

Comparison of the kinematics of the pelvis and lower extremities using the various arm slings (P<0.05)
Pelvic rotation amplitude in less-affected side at stance phase (*P<0.05).

Changes of the less-affected knee kinematics at minimal value (*P<0.05).
The activities of the anterior and posterior deltoid and latissimus dorsi muscles did not differ significantly while walking using the various arm slings (Table 3).

Comparison of the muscle activities in the affected side among the several arm slings (P<0.05)
DISCUSSION
We investigated the effects of a flexed arm sling, extended arm sling, elastic arm sling, and no arm sling on kinematic data during gait, and the muscle activity of the arm in stroke patients.
The amplitude of pelvic rotation on the less-affected side significantly differed between the extended sling and both the flexed sling and no sling in the stance phase. In healthy people, the standard range of pelvic amplitude is about 10°, and maximal forward and backward rotation are about 5° during initial contact and terminal stance (Perry and Burnfield, 2010). In our study, the rotation on the less-affected side was about 7° without an arm sling and with a flexed arm sling, but was approximately 12° with an extended arm sling. By comparison, there was no significant difference between the elastic arm sling and the other slings. We hypothesised that the sling’s flexible elastic material plays a role similar to that of muscle, but further studies are needed.
The extended arm sling may provide stability to the contralateral shoulder, increasing the amplitude of pelvic rotation on the less-affected side. Indeed, some researchers have found that using additional arm weights increases shoulder stability and pelvic rotation (Yoon et al., 2016). In a study that compared the flexed and extended arm slings, the latter did not interrupt the arm swing, which plays an important role in counterbalancing the movement of the pelvis and lower extremities (Zehr and Duysens, 2004). In addition, the alignment of the glenohumeral joint in the paretic arm may be assisted by the extended arm sling (Dieruf et al., 2005).
A previous study of the elastic arm sling found that while it significantly improved walking velocity and both step and stride length, there was no significant difference in pelvic rotation amplitude (Hwang and An, 2015). We postulated that the elastic tension would provide flexibility as well as stability for support. Therefore, an elastic arm sling with tension may aid gait training in stroke patients.
Yavuzer and Ergin (2002) found that the kinematics of arm rotation did not significantly differ between using a flexed arm sling and not using one. Our results are in agreement. The flexion pattern of the upper extremity did not differ from kinematic data without an arm sling. However, research has shown that a flexed arm sling can increase walking speed, double the stance period, and increase weight-bearing on the paretic side (Yavuzer and Ergin, 2002). The kinematics of the less-affected knee differed significantly between each sling and not using one. The stability of the contralateral shoulder with the slings might help to extend the knee on the less-affected side. Anatomically, if we consider the spiral line of fascial connections to the rhomboids major and minor, the lower part of the serratus anterior, the external oblique, and the opposite of the internal oblique (Myers, 2014), then all of the arm slings might enhance the stability of the trunk, which in turn might enhance knee extension. In addition, the vertical movement produced by the restrained arm swing using an arm sling increases knee extension (minimal knee kinematics), because lower swings of the counteracting arm result in higher vertical moment (Li et al., 2001). However, a recent study found that flexed and extended arm slings had no effect on balance, including weight asymmetry patterns, although the stroke patients were standing in that investigation (Sohn et al., 2015). In addition, unlike our study, those researchers applied a Bobath sling to both the affected and unaffected sides.
We investigated the effects of changes in the muscle activity of the swinging arm on stability during walking while wearing flexed, extended, and elastic arm slings. There were no differences in muscle flexion or extension of the affected arm. A reciprocal arm swing is a natural motion during walking (Perry and Burnfield, 2010), and we inferred that an arm sling does not interrupt the automatic arm swing response. In the neural system, a locomotor pattern generator may control arm swing (Jackson et al., 1978). Gutnik et al. (2005) compared arms with simple and unrestrained pendulums. Symans and Constantinou (1999) considered the passive arm swing to act as a mass damper system that transfers energy from the swinging legs and spinal column. However, Ballesteros et al. (1965) suggested that the muscle activity in the shoulder plays an important role in maintaining stability while walking and especially while running.
This study had some limitations. The sample size was too small to normalise the kinematic data, and arm swing motion with different arm slings was not evaluated. Muscle activity was not compared between the anteversion and retroversion of the arm swing. We evaluated the kinematic data of the lower extremities while walking and wearing various arm slings. Further studies should investigate the effects of arm slings to research arm kinematics and arm swing.
In stroke patients, an extended arm sling has a greater effect on pelvic rotation on the less-affected side than no sling or a flexed arm sling in the stance phase during walking. Without a sling, the less-affected knee joint is flexed more than with any sling. All arm slings tested supported the extension of the contralateral knee.
ACKNOWLEDGMENTS
This study was funded from Hoseo University, Asan, South Korea (2016-0062). Thanks to the Haundae Baek and Seo-ho Hopstital, we could investigate this study.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.