Effect of timing of whey protein supplement on muscle damage markers after eccentric exercise
Article information

Abstract
Whey protein is a nutritional supplement commonly ingested for recovery following exercise. However, the timing when whey protein supplement must be ingested after muscle-damaging exercise is debatable. Therefore, the present study investigated the effects of the timing of supplement ingestion on muscle damage markers after eccentric or muscle-damaging exercise. In total, 32 collegiate male students participated in this study; they were randomly assigned to control group (n=8), before supplement group (n=8), after supplement group (n=8), or before and after supplement group (n=8). Eccentric exercise was performed using elbow flexors with a modified preacher curl machine. Subsequently, maximal isometric strength, muscle soreness, range of motion (relaxed and flexed arm angle), and blood markers (creatine kinase and aspartate transaminase) were measured before and after exercise. Repeated-measure analysis of variance was used to analyze the effects of timing of supplement. No significant group by time effects were noted in maximal isometric strength, muscle soreness, range of motion, and blood markers (P>0.05). The timing of whey protein supplement did not affect reduction of muscle damage or recovery following eccentric exercise.
INTRODUCTION
It is well known that repeated high-force eccentric exercise induces muscle damage (Chen et al., 2011). Muscle damage reduces maximal isometric strength and range of motion (ROM) and increases muscle soreness and blood markers such as creatine kinase (CK) (Clarkson and Hubal, 2002). In addition, damaged muscle tissue results in muscle degeneration by degradation of structural proteins, including myofibrils and cytoskeletal proteins (Phillips et al., 1997). Whey protein is commonly ingested after exercise, and it has been used as a supplement to prevent muscle degeneration and to increase protein synthesis (Cooke et al., 2010). Whey protein is a protein extract from coagulation by-products when milk is coagulated during the process of cheese production and includes several essential amino acids that are easily digested and absorbed (Mahé et al., 1996).
Several studies have reported that whey protein supplements after exercise are beneficial to facilitate recovery by increasing protein synthesis and reducing muscle damage (Buckley et al., 2010; Cooke et al., 2010). In contrast, whey protein supplements before resistance exercise has been reported to increase protein synthesis and muscle regeneration (Witard et al., 2009). In addition, consumption of protein supplements rich in essential amino acids before resistance exercise had greater effects on amino acids levels and protein synthesis than did their consumption after exercise (Tipton et al., 2001). On the other hand, a recent study showed that whey protein supplements before and after exercise promoted recovery from resistance exercise (Hoffman et al., 2010). Based on results of previous studies where the type of exercise was mostly resistance exercise, which may not always induce muscle damage, it is unclear whether the timing of whey protein supplement might have any effect on reduction of muscle damage or recovery from muscle-damaging exercise. Therefore, the present study investigated the effects of the timing of whey protein supplement ingestion on muscle damage markers following eccentric exercise.
MATERIALS AND METHODS
Subjects
In total, 32 male collegiate students who had not participated in any exercise program in the past 6 months, were nonsmokers, and had not consumed any supplements with protein or vitamin products were included in the study. Each subject was explained the purpose of the study as well as all study procedures before obtaining a signed informed consent form. Each subject was randomly assigned to either control, before supplement group (BSG), after supplement group (ASG), or before and after supplement group (MSG). Subject characteristics are summarized in Table 1.

Characteristics of subjects
Body composition
Body composition was measured using a bioelectrical impedance instrument (InBody 520, Biospace, Seoul, Korea). Before measurement, each subject was requested to fast overnight and to abstain from intense exercise or sauna.
Whey protein supplement
Whey protein supplement was ingested in powder form (1.5 g/kg) mixed with 300 mL of plain water. BSG was supplemented 10 min before exercise, ASG 10 min after exercise, and MSG 10 min before and after exercise. The control group did not ingest any supplement during the experiment. Each subject was requested to ingest ordinary meals until the experiment was completed and to abstain from excess protein consumption. Each subject recorded his daily dietary intake and was requested to submit these records at the end of the experiment.
Eccentric exercise
Eccentric exercise comprised two sets of 25 eccentric contractions of elbow flexors by using a modified preacher curl machine, wherein each subject was seated on the machine with his chest and arm placed on the pad. While the investigator pushed down the lever attached to the machine, each subject pulled his arm maximally to perform eccentric contractions (Clarkson et al., 2005).
Maximal isometric strength
Maximal isometric strength of the elbow flexors was recorded using a strain gauge (PKS-1250, Poong Kwang, Seoul, Korea) attached to the modified preacher curl machine. Three sets of measurements were recorded each before, immediately after and 24, 48, 72, and 96 hr after exercise.
Muscle soreness
Muscle soreness was determined using a visual analog scale, wherein 0 indicated no soreness and 10 indicated severe soreness. Muscle soreness was measured before and 24, 48, 72, and 96 hr after exercise.
Range of motion
ROM was measured using a goniometer (S29-5900, KASCO, Islamabad, Pakistan). Both relaxed- and flexed-arm angles were measured when the elbow was completely relaxed and flexed, respectively, before, immediately after and 24, 48, 72, and 96 hr after exercise.
Blood markers
Blood samples (5 mL) were obtained from antecubital vein before and 24, 48, 72, and 96 hr after exercise to analyze CK and aspartate transaminase. In order to collect serum, sample vials were centrifuged at approximately 2,500–3,000 rpm; subsequently, the serum was transferred into a microtube and stored at −80ºC in a freezer (Ultra-Low Temperature Freezer, OPERON, Gimpo, Korea) until these were evaluated in an automatic blood sample analyzer (DT60II, Johnson & Johnson, Minneapolis, MN, USA).
Statistical analysis
All parameters were indicated as mean and standard deviation. By using the IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA), repeated-measure analysis of variance was used to analyze the groups by time interactions. Significance was set at 0.05.
RESULTS
Maximal isometric strength and ROM were significantly reduced following eccentric exercise (P<0.001), while muscle soreness and blood markers were significantly increased after exercise (P<0.001). However, there were no significant effects of the timing of supplement ingestion on maximal isometric strength (P=0.516), ROM, muscle soreness (P=0.791), and blood markers following eccentric exercise. The results are presented in Tables 2–7.

Change of maximal isometric strength (%) after eccentric exercise

Change of muscle soreness (mm) after eccentric exercise

Change of relaxed arm angle (˚) after eccentric exercise

Change of flexed arm angle (˚) after eccentric exercise

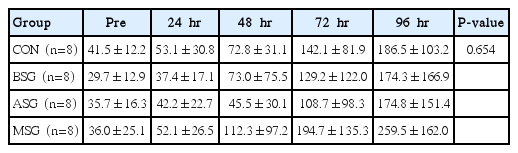
Change of creatine kinase (U/L) after eccentric exercise
Change of aspartate aminotransferase (U/L) after eccentric exercise
DISCUSSION
The present study investigated whether the timing of whey protein supplement can affect muscle damage markers after eccentric exercise; however, the results revealed no significant effects of the timing of ingestion on muscle damage markers after exercise. These results are not concordant with those reported in previous studies. Buckley et al. (2010) and Cooke et al. (2010) reported that whey protein supplements consumed after eccentric exercise resulted in faster recovery of muscle strength. However, there was a difference in the frequency of supplement ingestion between previous studies and the present study. In the study conducted by Buckley et al. (2010), subjects ingested whey protein immediately after and 6 and 24 hr after eccentric exercise, while the study by Cooke et al. (2010) revealed significant effects of whey protein supplement ingested 4 times/day for 2 weeks after eccentric exercise. However, in the present study, one dose each was ingested before, after, or before and after eccentric exercise. In fact, several studies with a single dose of whey protein supplement have reported results similar to those of our study. Burnley et al. (2010) reported that a single dose of whey protein supplement after eccentric exercise did not improve muscle soreness and CK activity. In addition, White et al. (2008) reported that whey protein supplement before or after eccentric exercise did not influence any muscle damage markers. In contrast, a recent study demonstrated that whey protein supplement consumed after eccentric exercise for 7 days resulted in increased fibroblast proliferation and faster muscle strength recovery after exercise. This implies that the period of supplementation may be more important than the timing of supplement ingestion.
The difference between the present study and other previous studies may be attributed to the exercise protocol used in this study. Eccentric exercise with elbow flexors is known to produce greater muscle damage (Jamurtas et al., 2005) compared with exercise protocols with lower limb that use an isokinetic dynamometer or downhill running or walking on a treadmill (Jamurtas et al., 2005; Tiidus, 2008). Most previous studies had used isokinetic eccentric contractions of the lower limb (Buckley et al., 2010; Cooke et al., 2010; Dale et al., 2015). Moreover, certain other studies on effects of whey protein supplements had used lower-limb resistance exercises (Hoffman et al., 2010; Tipton et al., 2011; Witard et al., 2009). For instance, Buckley et al. (2010) reported that peak CK activity at 24 hr after eccentric exercise ranged 196.5–386.8 U/L, while Hoffman et al. (2010) reported that the peak CK activity did not reach 250 U/L at 48 hr after resistance exercise. In the present study, CK activity at 24 hr after eccentric exercise ranged 440–2,175 U/L.
Greater muscle damage leading to protein degradation may require higher protein intake during the recovery period (Phillips and Van Loon, 2011). A universal resistance exercise also induces increased protein degradation until up to 48 hr after exercise (Phillips et al., 1997). Therefore, sufficient intake of amino acids in the form of protein supplements is required to delay protein degradation and promote protein synthesis (Wagenmakers, 1999). In contrast, insufficient protein intake may delay recovery after exercise by increasing protein degradation, leading to a negative nitrogen balance (Rennie and Tipton, 2000).
In conclusion, a single dose of whey protein supplement, regardless of the timing of supplement ingestion, may not be beneficial after muscle-damaging exercise.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.