Motor proficiency differences among students with intellectual disabilities, autism, and developmental disability
Article information

Abstract
There is considerable overlap in the manifestations of intellectual disability, autism, and developmental disability. We aimed to determine whether students with such disabilities have differences in their motor proficiency. We compared the motor proficiency of 82 students (age, 11 to 20 years) with different severities of intellectual disability (borderline, 11 students; mild, 27 students; moderate, 19 students), developmental disability (15 students), or autism (10 students). The Bruininks-Oseretsky Test of Motor Proficiency, Second edition was used to assess motor skills. The data were analyzed using descriptive statistics, independent t-tests, and analysis of variance. Compared to students with borderline intellectual disabilities, mild intellectual disabilities, or autism, those with moderate intellectual disabilities scored significantly lower on al-most all items regarding motor skill on the Bruininks-Oseretsky Test of Motor Proficiency. The results of this study provide key information for developing exercise programs to improve the motor proficiency and quality of life of children with various developmental disorders.
INTRODUCTION
A recent report of the Korea Institute for Health and Social Affairs (2014) indicated that, in Korea, 183,868 students have developmental disability developmental disability and/or intellectual disability, including autism and borderline intellectual disability (intelligence quotient [IQ]=71 to 79). While there are differences between developmental disability, intellectual disability, and autism, all such conditions are characterized by deficits in 3 developmental areas, including language and communication, restricted patterns of behaviors of interest, and social interactions (American Psychiatric Association, 2013). Intellectual disability is known as a general learning disability, while mental retardation is considered as a generalized neurodevelopmental disorder characterized by significant limitations in both intellectual and adaptive functioning, an IQ<70, and deficits in 2 or more adaptive behaviors covering many everyday social and practical skills (American Association on Intellectual and Developmental Disabilities, 2018). Individuals with mild intellectual disability can generally acquire reading, writing, and mathematics skills to the level of grade 3 to 6, often enabling them to hold jobs and live independently. Individuals with moderate intellectual disability can also learn some basic reading and writing skills, but functional skills, such as those related to safety and self-help, require some form of oversight or supervision. A developmental disability is a severe chronic disability of a cognitive and/or physical nature that manifests before the age of 22 years. Individuals with developmental disability face several challenges, especially with respect to language, mobility, learning, self-help, and independent living. A developmental disability that affects all areas of a child’s development is sometimes referred to as a global developmental delay (Centers for Disease Control and Prevention, 2013).
Autism is a neurodevelopmental disorder characterized by impaired social interaction and cognitive capabilities, communication difficulties, and repetitive behaviors (Landa, 2008; National Autism Association, 2017). Some studies have demonstrated that individuals with autism have delayed development compared to that of students of the same age without the disability (Staples and Reid, 2010).
Individuals with the disorders outlined above also exhibit delayed achievement of motor milestones as well as impaired sensorimotor function (Hogan et al., 2000), poor movement control, motor sequencing deficits, specific verbal-motor difficulties, poor comprehension, and low concentration (Charlton et al., 2000; Maraj et al., 2003; Piek et al., 2012; Uyanik et al., 2003). Motor and social interaction skills are needed in order to perform purposeful activities in daily life. Motor skills are defined as the goal-directed actions a person enacts when interacting with and moving task objects and themselves around a task environment (Hartman et al., 2010; Jurado and Rosselli, 2007). Cognitive development relies on motor function, and recent findings also suggest that motor performance and high-order cognitive functions (e.g., executive functions) are related (Diamond, 2000; Piaget and Inhelder, 1966; Ridler et al., 2006; Wassenberg et al., 2005). Well-developed motor skills are important because they are thought to facilitate a child’s cognitive development, contribute positively to activities of daily living, and serve as building blocks for the development of more complex motor and sports-specific skills (Piek et al., 2008; Smits-Engelsman and Hill, 2012; Stodden et al., 2008; Wall, 2004). The poor motor performance observed in children with borderline and mild intellectual disability is believed to be caused also by their impaired intellectual capabilities. Furthermore, exclusion from physical activity hinders a child’s physical, psychological, and social development and can have a negative influence on future sports participation and physical activity. Motor proficiency in childhood has been shown to influence participation in physical activity, and increased physical activity in childhood is associated with positive health outcomes (Fisher et al., 2005; Frey and Chow, 2006; Ulrich, 2000; Westendorp, 2011).
Several studies have reported that motor problems and low motor proficiency are associated with negative consequences such as the avoidance of physical activity, obesity, lack of concentration, low self-esteem, poor academic performance, and poor social competence (Wuang et al., 2008). It is considered important for children to participate in physical activity for their enjoyment, well- being, physical fitness, health, and social development, as children who exercise have a lower likelihood of becoming obese and a reduced risk of cardiovascular disease (Capio et al., 2015; Piek et al., 2012). Furthermore, reduced participation in regular sports activities and a lack of exercise lead to a “negative spiral of engagement” in children with low motor proficiency (Capio and Rotor, 2010; Gallahue and Ozmun, 2002; Hardy et al., 2010; Williams et al., 2008).
The Bruininks-Oseretsky Test of Motor Proficiency-Second Edition (BOTMP-2) is widely used to assess an array of motor skills for both clinical and research purposes. The BOTMP-2 is designed for subjects aged 4 to 21 years and consists of 8 subtests that are further organized into 4 composites according to the muscle groups and limbs involved in the task movements. The BOTMP-2 provides clinicians, educators, and researchers with useful information to assist them in evaluating the motor proficiency of students. The BOTMP-2 allows the assessment of students with normal development as well as the assessment of those with up to moderate motor skill deficits (Bruininks and Bruininks, 2005; Wuang et al., 2008), providing information about which sports and activities students should practice or avoid and which specific skills and coordinated movements they need to develop (Ekelund et al., 2004; Okely and Booth, 2004; Strong et al., 2005).
Few studies have examined the motor proficiency of students with borderline or mild intellectual disability, developmental disability, and autism. It is possible that there are differences in motor proficiency among students with such conditions. Therefore, it is necessary to improve our understanding of the motor proficiency level and pattern in children with borderline, moderate, or mild intellectual disability, developmental disability, and autism. In this context, the purpose of the present study was to evaluate the BOTMP-2 scores of male students with intellectual disability, developmental disability, or autism and to elucidate the differences in motor skills among the students with such disorders.
MATERIALS AND METHODS
Participants
The participants were recruited and evaluated at Gachon University’s exercise rehabilitation department. Eighty-two male students with autism, developmental disability, or intellectual disability participated in the study. We divided the students into 5 groups based on whether they were diagnosed with moderate intellectual disability (IQ=35 to 49), mild intellectual disability (IQ=50 to 70), borderline intellectual disability (IQ=71 to 79), developmental disability, or autism.
In total, we included 19 students with moderate intellectual disability, 27 students with mild intellectual disability, 11 students with borderline intellectual disability, 15 students with developmental disability, and 10 students with autism. All participants attended special needs education or mainstream schools in the same city. The study was conducted from April 2015 to November 2015. The 5 groups (moderate intellectual disability, mild intellectual disability, borderline intellectual disability, developmental disability, and autism) did not differ significantly with respect to age (F=1.66, P=0.885). The legal guardians provided informed consent for the students to participate in the study, and all procedures were conducted in accordance with Gachon University’s ethical standards.
Evaluation tool and testing procedure
To assess the participants’ motor performance, we used the BOTMP-2, a normative referenced standard motor assessment test available as a form with 53 items (Bruininks and Bruininks, 2005). The BOTMP-2 version used in our study consists of 4 composite motor domains: fine manual control, which includes fine motor precision (41 points) and fine motor integration (40 points); manual coordination, which includes manual dexterity (45 points) and upper limb coordination (39 points); body coordination, which includes bilateral coordination (24 points) and balance (37 points); and strength and agility, which includes running speed and agility (52 points) and strength (42 points). The total BOTMP-2 motor proficiency score is 320. The researchers rated each participant on each subtest item. For each group, the average scores and the mean rate of mastery were calculated for each subtest, each composite, and the overall motor BOTMP-2 test.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA), and the significance level was set at 0.05. Total motor proficiency composite scores, subtest raw scores, and specific raw scores were set as the dependent variables. We used descriptive statistics, independent t-tests, and analysis of variance (ANOVA) to compare the groups in terms of total scores as well as in terms of the subtest scores for motor proficiency, fine motor manual control, manual coordination, body coordination, strength, and agility. We used linear regression to correct for the influence of age.
RESULTS
There were no significant differences in mean age (P=0.885) among the five groups (Table 1). However, ANOVA indicated significant differences among the groups in terms of mean standard scores for the total motor composite, four motor-area composites, and eight subtest scores (Table 2). The mean rate of mastery of motor proficiency was 38.96% in children with moderate intellectual disability, 47.4% in those with developmental disability, 58.65% in those with autism, 58.78% in those with mild intellectual disability, and 68.8% in those with borderline intellectual disability (Table 1). Regarding the four motor-area composites, in all groups, mastery achievement rates were highest for fine manual control and lowest for strength and agility (Table 2).

Characteristics of the study participants
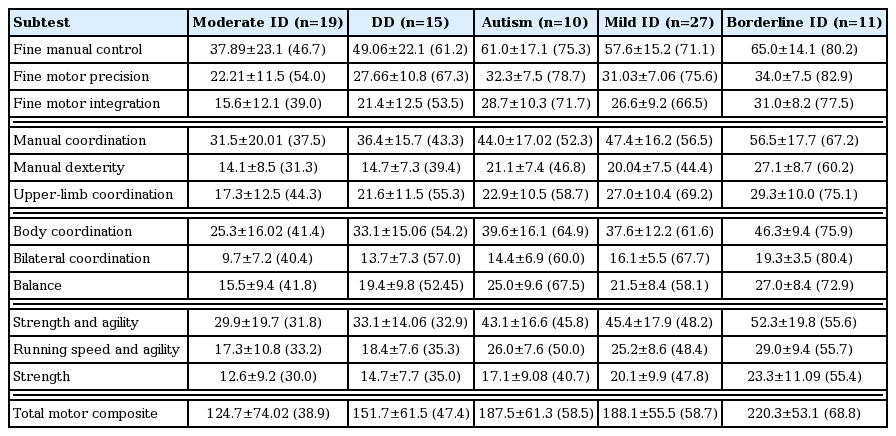
Estimated motor proficiency for each subtest of the Bruininks-Oseretsky test of motor proficiency, second edition
There were no differences between students with moderate intellectual disability and developmental disability with respect to the total motor composite, each motor-area composite, or subtest scores. Compared to moderate intellectual disability, autism was associated with significantly higher scores for fine manual control, fine motor precision, fine motor integration, manual dexterity, body coordination, balance, strength and agility, strength, and total motor composite. Compared to moderate intellectual disability, both mild intellectual disability and borderline intellectual disability were associated with significantly higher scores for the total motor composite, each of the four motor-area composites, and each subtest (Table 3). Compared to the developmental disability group: (a) the autism group had significantly higher scores for manual dexterity, running speed, and agility; (b) the mild intellectual disability group had higher scores for manual coordination, manual dexterity, strength and agility, running speed, and agility; and (c) the borderline intellectual disability group had higher scores fine manual control, fine motor integration, manual coordination, manual dexterity, body coordination, bilateral coordination, balance, strength and agility, running speed and agility, strength, and total motor composite (Table 3). Compared to mild intellectual disability, borderline intellectual disability was associated with significantly higher scores for manual dexterity and body coordination (Table 3). There were no significant differences between the autism group and the mild intellectual disability group or between the autism group and the borderline intellectual disability group.
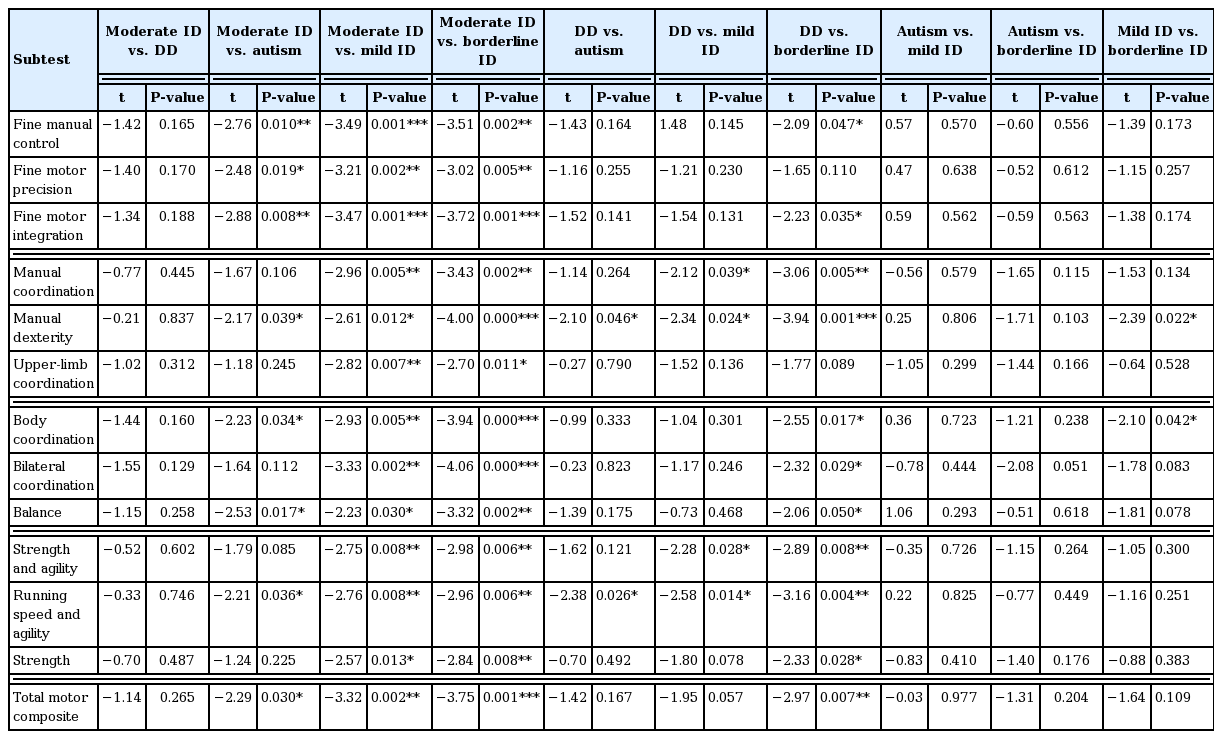
Comparison of motor proficiency according to disability
DISCUSSION
In this study, which enrolled 11- to 20-year-old male students with developmental disability, intellectual disability, or autism, we found an overall mastery rate of 54.5% for motor proficiency. Compared to their borderline intellectual disability counterparts, students with developmental disability, autism, mild intellectual disability, or moderate intellectual disability scored significantly lower on the motor proficiency 4-area composite and subtests of the BOTMP-2. We also found that these students scored higher for fine manual control but lower for strength and agility.
The study by Gaul and Issartel (2016) showed that, compared to children with developmental disability, those with intellectual disability have worse fine motor skills. Westendorp et al. (2011) showed that children with mild intellectual disability or borderline intellectual disability have impaired motor skills compared to those of children who develop normally and found no difference between children with mild intellectual disability and those with borderline intellectual disability in terms of gross motor skills. These previous results are not in agreement with the findings of the present study. While poor cognitive proficiency appears to be the most pertinent concern, students with borderline and mild intellectual disability have also been found to have worse motor skill performance than children without developmental impairment (Westendorp et al., 2011). Our present finding that children with intellectual disability had lower gross motor skill scores is consistent with the observations of Frey and Chow (2006).
Interestingly, we did not find significant differences between students with developmental disability and those with moderate intellectual disability in all areas of motor proficiency. Specifically, students with moderate intellectual disability had worse scores than those of students with autism for fine motor precision, fine motor integration, and manual dexterity. On the other hand, students with moderate intellectual disability showed worse deficits than those with mild intellectual disability in all areas of the BOTMP-2. Westendorp et al. (2011) studied children with mild intellectual disability and borderline intellectual disability and found no differences in object control between the groups but revealed that all participants performed better at leaping, jumping, and sliding actions of locomotion. While Westendorp et al. (2011) used the Test of Gross Motor Development-2 and not the BOTMP-2, their conclusions are similar to ours.
In this study, there were no significant differences between mild intellectual disability and autism or between autism and borderline intellectual disability. Based on the results of this study, performance in all areas of BOTMP-2 seems more likely to be related to IQ than with the type of disability (intellectual disability, developmental disability, or autism). Casey et al. (2005) and Wuang et al. (2008) found that IQ and cognitive function affects motor performance (Choi and Roh, 2011). Although we did not perform IQ tests, we also believe that BOTMP-2 performance is related to IQ because the variations in motor proficiency between children with different degrees of intellectual disability (moderate, mild, and borderline) confirm the findings of previous studies that IQ and cognitive abilities are related to motor performance.
Children with intellectual disability have impaired sensorimotor skills (Wuang et al., 2008) and developmental retardation of the central nervous system, likely related to the fact that motor control emerges from the complex interaction of cognitive sensory and motor systems in the brain (Casey et al., 2005). Indeed, children with mild intellectual disability display sensory integrative dysfunction, particularly in integrative areas of sensory discrimination and sensory searching. These sensory processing deficiencies may contribute to the adaptive behavior deficits of these children and may impact their ability to engage in home, educational, and social activities.
Total IQ is recognized as a robust predictor of the quantitative and qualitative aspects of motor behavior as well as graphomotor skills, as outlined in the perspectives put forth by Piaget and Inhelder (1966) and von Hofsten (2004, 2007) However, the findings of Wassenberg et al. (2005) are partially contradictory, as they maintain that general cognitive performance is relevant in predicting qualitative rather than quantitative aspects of movement. One of the sources for this discrepancy regarding our understanding of the principles underlying motor development is the increasingly prominent role that technology plays in the modern society. A number of studies have shown how children develop in the current, media-saturated environment, with technology playing a central role in their daily lives. In the present study, fine motor performance was less impaired than strength or agility performance, indicating that the children investigated had reduced levels of physical fitness and, potentially, worse health. This finding could highlight the importance of physical exercise for children with intellectual disability, developmental disability, or autism in order to improve or maintain their health and wellbeing, particularly in the context of the changes in behavior related to the use of technology, as outlined above.
The key limitation of the present study is that we did not assess IQ directly and instead obtained the relevant data from the parents. Further studies involving meticulous IQ tests are warranted to verify the relationship between IQ and motor skill performance in children with intellectual disability, developmental disability, or autism.
In conclusion, the present results showed that school-aged children with moderate intellectual disability performed worse than children with borderline intellectual disability or mild intellectual disability in all motor proficiency areas. Furthermore, students with moderate intellectual disability scored lower than those with autism in all motor proficiency areas except for manual coordination, upper-limb coordination, bilateral coordination, strength and agility, and strength. The students with developmental disability performed worse than those with borderline intellectual disability in all motor proficiency areas except for fine motor precision and upper limb coordination. The present results are contrary to those of previous studies and highlight the need for further study in this area.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.