Functional resistance training can increase strength, knee torque ratio, and functional performance in elderly women
Article information

Abstract
Functional resistance training can increase strength, knee torque ratio, and functional performance in elderly women. The aim of the present study was to understand the effects of closed kinetic chain exercises with constant load on muscular strength, the knee torque conventional ratio (hamstring:quadriceps – H:Q), and functional capacity in the elderly. Nine untrained healthy elderly women participated in experimental resistance training. Ten-repetition maximum (10RM) for the deadlift, isokinetic maximum voluntary concentric contraction, and functional capacity were assessed before and after the 7-week resistance-training program. Magnitude based inference analysis was used to examine the differences in muscle strength and functional performance. Therefore, the smallest worthwhile change was calculated and 90% confidence intervals were also determined to characterize muscle strength and functional performance. The analysis demonstrated an increase in the deadlift and knee flexor torque (60o/sec) after the experimental intervention. Furthermore, stair ascent, knee extensor torque (120o/sec), knee flexor torque (120o/sec), and knee ratio (60o/sec) also presented a positive effect in the same training period. Conversely, knee extensor torque (60o/sec), and knee ratio (120o/sec) did not show conclusive responses. In conclusion, resistance training with functional closed kinetic chain exercises and constant volume load (i.e., 65% of 1-repetition maximum) can increase deadlift 10RM, isokinetic concentric torque, the conventional H:Q ratio, and stair ascent performance in elderly women.
INTRODUCTION
Aging is associated with the process of reduction in strength and muscle mass (Manini and Clark, 2012). This process has a high impact on the reduction in the capacity to perform daily living activities (e.g., walking, sitting, and stair negotiation) and an increased risk of falls in elderly populations (Scott et al., 2015). Furthermore, women appear to be affected earlier and to a greater magnitude than men (Leyva et al., 2016). Among all strategies for increasing strength and improving functional ability in the elderly, resistance training has been shown to be a safe and effective intervention (Borde et al., 2015; Byrne et al., 2016; Steib et al., 2010). However, resistance training involves a great number of variables, such as: muscle action, rest periods, repetition velocity, frequency, exercise selection and order; and loading and volume (Bird et al., 2005).
In addition, the loading and volume interplay has been reported as a critical factor for positive effects on strength gains in different populations (Fisher et al., 2013; Fisher et al., 2017; Schoenfeld, 2013), as well as which loading and volume can determine the optimal range of training. In particular the loading and volume interplay is based on the training principle of progression; it indicates the necessity to change the load volume in resistance training programme designs (Bird et al., 2005).
For improvements in muscular strength in older subjects, the American College of Sports Medicine recommends the use of intensities between 60%–80% of one-repetition maximum (1RM) and moderate to slow contraction velocity (Ratamess et al., 2009). Moreover, a recent meta-analysis (Borde et al., 2015; Steib et al., 2010) suggests that higher intensities result in greater improvements in strength compared to moderate intensities. However, the use of greater intensities in untrained elderly individuals requires longer periods of recovery for neuromuscular (i.e., explosive force, power, and strength) resistance training-related acute impairments, exposing the elderly to reduced balance and functional capacity and an increased risk of falling (Orssatto et al., 2018a). Following this rationale, lower intensities (i.e., ~60% of 1RM) would be safer and efficient for strength increases for untrained elderly, while the intensity could be gradually increased in subsequent months of training.
Conversely, the elderly require increases in functional capacity, while Walker et al. (2017) suggested that training intensities of ~50%–60% and slow contraction velocities did not provide improvements in functional capacity. However, it can be hypothesized that these results could be explained by the exercise choice, and not by the adopted intensity. The cited study adopted nonfunctional exercises for lower limbs (i.e., horizontal leg press, knee extension, and knee flexion), which do not follow the movement pattern specificity of daily living activities. In this context, the choice of multi-articular and closed kinetic chain functional exercises, such as the squat or deadlift (more related to daily living movements), would result in improvements in functional capacity beyond strength in the elderly. Despite these exercises being considered functional and involving activation of knee extensors and flexors (Escamilla et al., 2001), it is unclear in the literature if the increases in strength between knee antagonist muscles is similar. For example, recently Orssatto et al. (2018b) reported increases in knee extension but not knee flexion torque that consequently reduced knee torque ratio, after 12 weeks of resistance training using the leg press, which is characterized by participation of both knee extensors and knee flexors (Walker et al., 2011).
Thus, the aim of the present study was to understand the effects of closed kinetic chain exercises with constant load on muscular strength, the knee torque conventional ratio, and functional capacity in the elderly.
MATERIALS AND METHODS
Experimental design
The study design was a pre-post nonrandomized design. During the first visit, subjects were informed about the study design, procedures, and performed body mass and height assessments. On the subsequent three days, each one separated by 48 hr, subjects performed familiarization sessions. 48 hr after the familiarization period, the subjects attended two visits, each separated by a minimum of 48 hr, during which they were tested and retested for baseline values in: (a) Isokinetic maximum voluntary concentric contraction, (b) functional capacity, and (c) ten-repetitions maximum (10RM). After testing, subjects started the resistance training program. Thereafter (posttraining), each subject completed the same tests performed at baseline.
Subjects
Subjects completed a health history and physical activity questionnaire. Participants were required to meet the following inclusion criteria: ≥60 years old, physically independent, free from cardiac disease, free from orthopaedic dysfunction, and not having performed noncontrolled physical activity within one year preceding the beginning of the study. Fourteen women were initially eligible; however, after the intervention period only nine subjects (70.7±6.5 kg; 1.53±0.03 m; 64.1±2.1 years) completed all stages of the experiment (i.e., five subjects dropped out). One subject withdrew claiming muscular discomfort during the resistance training regime and four did not reach the established minimum session attendance (frequency>85% [Gentil and Bottaro, 2013]). Adhesion to the program was satisfactory, with all subjects participating in ≥13 (>90%) of the total sessions. Written informed consent was obtained from all subjects after providing a detailed description of study procedures. All procedures performed in this study were approved by a local Institutional Ethics Committee (approval number: 1.753.546) and followed the ethical guidelines of the Declaration of Helsinki (64th World Medical Association General Assembly, Fortaleza, Brazil, October 2013).
Physical performance tests
Subjects performed a 10RM test in the deadlift exercise. Tests’ quality control was adapted from Orssatto et al. (2018a) study procedures. Knee joint range of motion was standardized from ~90° to ~5° of flexion during the deadlift measured by a goniometer. Using the same equipment and settings, the same evaluator conducted the familiarization, pre- and posttests. To ensure that the true 10RM was reached, subjects were encouraged to perform an eleventh repetition after the tenth. Thus, if less than 10 repetitions were performed, the weight was reduced for the next trial, and if eleven repetitions were performed, the weight was increased. The 10RM test was considered successful when the subjects performed exactly 10 repetitions. Each subject performed 1–3 trials with a rest period of 5 min. All subjects performed a specific leg press warm up (50% load performed in the final familiarization session) before starting the 10RM test.
Concentric knee extensor and flexor peak torques of the preferred limb were assessed on an isokinetic dynamometer (Biodex System 4 Pro, Biodex Medical Systems, Shirley, NY, USA). The subjects were seated at 70° and 90° for hip and knee angle joints, respectively (0° 1/4 knee fully extend). Subjects were verbally encouraged to perform three maximum concentric knee extensor (QCON) and flexor (HCON) contractions at 60°/sec and 120°/sec isokinetic velocity. A 3-min rest period was allowed between trials. The highest torque value for each test was used for data analysis. Stair ascent was assessed according to Rikli and Jones (2013). Each subject performed two attempts at each test and the fastest time was used for further analyses.
Resistance training program
At the beginning of each training session, subjects performed a general warm-up routine (treadmill walking [10 min], core training [2 sets of traditional prone plank and supine bridge exercises {15-sec isometric contraction per set} and one set with 50% of workout load for the first lower limb exercise]). Next, they performed the deadlift and free squat in all training sessions; the order of these exercises was alternated. The training intervention was completed with the same load (65% of estimated 1RM [Brzycki, 1993]) and 3 sets of 8–10 repetitions with a rest interval of 2 min between sets. The intervention protocol included 14 sessions (two sessions per week). The cadence of exercise was 2 sec for both the concentric and eccentric phases. Following the performance of lower limb training, a further complementary upper-body program was performed, consisting of 3 sets of 8–10 repetitions of the bench press and anterior lat pull down with a 2-min rest between sets. During all sessions, subjects were directly supervised (i.e., strength and conditioning trainers) to help ensure consistent and safe performance.
Statistical analyses
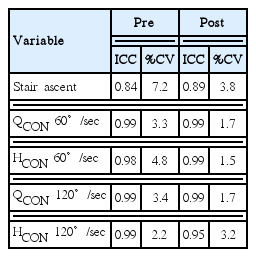
Magnitude based inference analysis was used to examine the differences in muscle strength and functional performance using a customized spreadsheet (Hopkins et al., 2009). The smallest worthwhile change was calculated (i.e., 0.2× by the between-subjects standard deviation [SD]) and 90% confidence intervals were determined to characterize muscle strength and functional performance (Hopkins et al., 2009). The quantitative chances of higher, similar, or lower differences were evaluated qualitatively as follows: <1%, almost certainly not; 1% to 5%, very unlikely; 5% to 25%, unlikely; 25% to 75%, possible; 75% to 95%, likely; 95% to 99%, very likely; >99%, almost certain. The true difference was assessed as unclear when the chances of having positive and negative results were both >5%. The threshold values for Cohen effect size (ES) statistics were >0.2 (small), >0.5 (moderate), and >0.8 (large). However, only differences classified as equal/higher likely and moderate ES were used as criteria for describing changes between groups. Values are reported as mean values ± and SD unless otherwise stated. Data reliability was calculated with the intraclass correlation coefficient and technical error (%CV) for the isokinetic and functional pre and post variables (Hopkins, 2000) (Table 1).
Data reliability
RESULTS
The analysis demonstrated an increase in the deadlift and knee flexor torque (60°/sec) after the experimental intervention. Furthermore, stair ascent, knee extensor torque (120°/sec), knee flexor torque (120°/sec), and knee ratio (60°/sec) also presented a positive effect in the same training period. Conversely, knee extensor torque (60°/sec) and knee ratio (120°/sec) did not show conclusive responses (Table 2, Fig. 1).
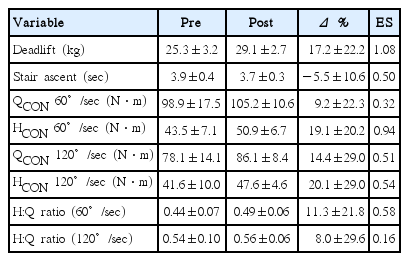
Pre and post mean±standard deviation, percentage changes (Δ %) and effect size (ES) for the assessed variables.
Magnitude based inferences for improvement (positive), reduction (negative), or inconclusive (trivial) in all experimental measures. Data are reported as (mean [post-pre] ±90% confidence limits). The smallest worthwhile change trivial zone was set at 20% of the pretraining standard deviation for each variable. 10RM, ten-repetition maximum; H:Q, hamstring:quadriceps; QCON, concentric knee extensor torque; HCON, concentric knee flexor torque.
DISCUSSION
The main findings in the present study suggest that the use of the deadlift and squat as functional exercises with constant load can improve muscular strength, knee conventional ratios, and functional capacity in elderly women. These results have relevant practical applications regarding exercise and training intensity prescription in this population.
The improvements in deadlift 10RM observed in the present study (~1.9% per week) are in agreement with several studies that adopted similar training intensities. For example, Walker et al. (2017) and Tsutsumi et al. (1998), respectively reported increases in leg press 1RM (+12%, ~1% per week) and knee extension 1RM (+36%, ~3% per week) with an intensity of ~50%–65% of 1RM, after 12 weeks of strength training. Additionally, Vincent et al. (2002) reported increases in leg press 1RM after 24 weeks (+17%, ~0.7% per week) with an intensity of 50% of 1RM.
Although a meta-analysis suggested that higher training intensities result in greater improvements in strength in the elderly, untrained elders are subject to acute neuromuscular impairments following resistance training, wherein higher intensities require longer recovery periods (Steib et al., 2010). During this recovery, the elderly seem to experience reduced ability to recover maximum torque, explosive torque, and power (Orssatto et al., 2018a) which are related to static as well dynamic balance (Izquierdo et al., 1999), thus increasing the risk of falling (Bento et al., 2010; Ema et al., 2016). Therefore, it would be safer to start the training program with intensities near 60% of 1RM and then increase the intensity gradually in subsequent months. The present study design resulted in chronic improvements in strength after 7 weeks of strength training without exposing the subjects to an increased risk of falling. Indeed, to ensure continuous improvements in strength it is necessary to increase intensity in subsequent weeks, when the repeated bout effect would protect the subjects and help to avoid exacerbated neuromuscular impairment following resistance training (Hyldahl et al., 2017; Orssatto et al., 2018a).
Another strength parameter assessed in the present study, the isokinetic concentric strength altered (QCON, 60°/sec=+0.9% and 120°/sec=+1.4%; and HCON, 60°/sec=+2.4% and 120°/sec=+2%, per week) and probably as a consequence the H:Q ratio (60°/sec) also changed (moderate ES). Our outcomes corroborate with other resistance training studies in the elderly. Orssatto et al. (2018b) reported significant increases of ~20% in QCON (60°/sec) peak torque (~1.7% per week) and nonsignificant increases of ~18% in HCON (60°/sec) peak torque (1.5% per week). One potential explanation for positive adaptation during constant volume load is that the deadlift and squat show high muscle activity in the biceps femoris (55%) and vastus lateralis (91%) during the maximum voluntary isometric contraction, respectively (Ebben et al., 2009), and these exercises were included in our resistance training programme with the same volume load.
Improvement in functional task performance has an important influence on the quality of life and reduces the risk of falling in the elderly (World Health Organization, 2007, 2015). Our result regarding stair ascent presented a positive response (moderate ES) even with no change in volume load. The exercises selected during the resistance training programme were the deadlift and squat, both of which require vertical centre of gravity displacement during the carrying of the load, and a similar displacement can be observed during stair ascent. Conversely, Walker et al. (2017) reported no statistical improvements in stair ascent after 12 weeks of resistance training using nonfunctional exercises (i.e., leg press, knee extension, and knee flexion exercises) and a similar intensity to that adopted in the present study (~50%–60% of 1RM). One indicative that exercise choice might play a role in functional capacity adaptations, is that MAT Pilates can improve stair ascent performance of elderly women after 6 weeks of training (Bertoli et al., 2017).
Strengths and limitations should be reported. Using the same experienced evaluator to perform all tests gives our study high internal validity. Another strength of the study is that we used a homogenous population of elderly unaccustomed to resistance training. On the other hand, the absence of a control group in the experimental design protocol does not enable an exact response. Furthermore, the results from the present study cannot be extrapolated to previously trained, older (e.g., >80 years), or frail subjects. Further studies should be developed with a larger sample size to confirm our findings.
As a practical application for resistance training prescription, trainers should consider the lack of necessity to adjust the intensity in the first weeks of resistance training for untrained elderly people, since this training includes closed kinetic chain exercises such as the squat and deadlift. Thereafter, training intensity can be increased gradually in subsequent weeks to ensure safety for daily living activities (Orssatto et al., 2018a). In conclusion, resistance training with functional closed kinetic chain exercises and constant volume load (i.e., 65% of 1RM) can increase deadlift 10RM, isokinetic concentric torque, the conventional H:Q ratio, and stair ascent performance of elderly women.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGMENTS
JOLS would like to thank the National Council for Scientific and Technological Development (CNPq) for the research fellowships to AB and EV, and MSc scholarship for LA. Furthermore, ESB would like to thank the Foundation for Research Support of the State of Amazonas (FAPEAM) for conceding a PhD scholarship.