Effect of resistance circuit training on health-related physical fitness, plasma lipid, and adiponectin in obese college students
Article information

Abstract
The purpose of this study is to investigate the effects of resistance circuit training on health-related physical fitness, plasma lipid and adiponectin in obese college students. Twenty male college students participated in this study and they were randomly divided into the sedentary group (SG, n=10) and the resistance circuit training group (RCG, n=10). The exercise group underwent the resistance circuit training program for 60 min 3 times a week for 12 weeks, while the sedentary group continued activities of daily living as usual. The levels of health-related fitness, blood lipid, and adiponectin were measured twice before and after the experiment. To analyze the statistically significance of collected data, Two-way repeated measure analysis of variance was used to determine the changes in the groups over the training period. A paired t-test was used to verify the difference within each group, and an independent t-test was used to verify the difference between the groups. In this study, the body composition including body fat mass, percent body fat and body mass index were significantly decreased in RCG compared to those in SG, and the health-related fitness showed a significant difference between RCG and SG. In addition, RCG positively modulated blood concentration of total cholesterol, triglycerides, high-density and low-density lipoprotein cholesterol. However, plasma adiponectin concentration did not show any significant differences between the two groups. Therefore, the present data suggested that resistance circuit training might be regulator to improve health-related physical fitness and decrease the level of plasma lipid in obese male college students.
INTRODUCTION
Obesity has been known as a complex disease involving an abnormal or excessive amount of body fat that may impair health (Upadhyay et al., 2018), and people who have been obese for long periods of time have a feeling of inferiority due to changes in body shape and deterioration of exercise capacity, and these changes lead to psychological problems along with passive activities. In addition, they have a high prevalence of various metabolic diseases, resulting in poor quality of life (Haslam and James, 2005; Zimmet et al., 2001). Among obese people of all ages, college students are highly dependent on favorite foods such as drinking and smoking, and they can easily become obese due to irregular meal times, job preparing stress, and lack of exercise (Peltzer et al., 2014). In specific, obese male college students have a lower awareness level of being obese than obese female college students, and have an optimistic perception that they are only overweight because obesity-related diseases or physical problems do not appear at their age. Therefore, obese male college students should seriously consider the risks to their health (Edman et al., 2005).
Metabolic diseases in obese people are closely associated with blood concentration of lipids including total cholesterol (TC), triglycerides (TG), high-density (HDL-C) and low-density (LDL-C) lipoprotein cholesterol (Tuomilehto, 2005). Hagey and Warren (2008) suggested that lowering TC and LDL-C concentration in the blood is effective in preventing various cardiovascular diseases in obese people, and Pines and Berry (2007) demonstrated the importance of regular exercise for reducing blood lipids.
In addition to blood lipids, recent studies have actively conducted research on the relationship between hormones secreted from adipocytes and metabolic disease in obesity. Adiponectin, leptin, interleukin-6 and tumor necrosis factor-alpha are a representative metabolic regulatory hormone secreted from the fat and/or adipose tissue. Adiponectin is a specific hormone induced only in adipocytes, and it is abundantly present in the blood. In addition, since adiponectin shows a negative correlation between visceral fat mass and visceral fat area, the blood concentration of adiponectin in obese people is lower than that of normal people (Kazumi et al., 2002). In some study on functional effect of adiponectin in obesity, adiponectin regulates glucose and lipid metabolism, and plays an important role in preventing cardiovascular disease by activating anti-inflammation mechanism (Arita et al., 2002). Esposito et al. (2003) reported that aerobic exercise for 2 years in obese middle-aged women resulted in a decrease in body weight (BW) along with an increase in plasm adiponectin concentration. Contrary to these positive effects of exercise on adiponectin levels in the blood of obese people, Hara et al. (2005) suggested that complex exercise for 8 weeks in obese adolescents did not induce changes in plasma adiponectin concentration, and Polak et al. (2006) reported that aerobic exercise for 12 weeks did not increase blood concentration of adiponectin in obese people.
Considering these research findings, the effect of exercise type, intensity and/or duration on blood adiponectin level in obese people remains controversial. Therefore, the purpose of this study was to investigate resistance circuit training for 12 weeks on health-related fitness, plasma lipid and adiponectin level in male college students with a body fat percentage of 25% or higher.
MATERIALS AND METHODS
Participants
The participants in this study were 20 obese male college students. As shown in Table 1, all participants were allocated to the sedentary group (SG, n=10) and the resistance circuit training group (RCG, n=10). Before beginning the measurement, participants were informed about study orally and they submitted their written informed consent to researchers. And this research was conducted ethically according to international guidelines. This research was approved by Ethical committee of Jeju National University (approval number: 2017-003-001).
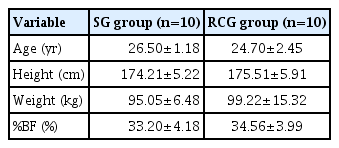
Physical characteristics of the subjects
Resistance circuit training program
Resistance circuit training program consisted of various machine and free weight exercises, and all subjects in RCG performed for 60 min 3 times a week for 12 weeks. The intensity of exercise was set as 40% of the one-repetition maximum (1RM) for 1–6 weeks, and 50% of 1RM for 7–12 weeks by applying indirect equation (1RM=weight lifted+[weight lifted×0.025×repetition]) for the estimation of 1RM. Resistance circuit training program in Table 2 was modified from the exercise program developed by Mayorga-Vega et al. (2013) and Rosety et al. (2016).
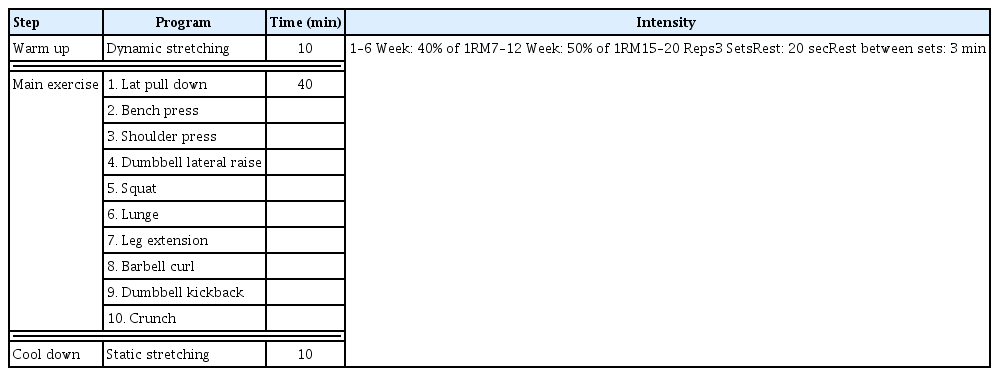
Resistance circuit weight training program
Body composition
The subjects visited the laboratory by 9:00 a.m. with 8 hours of fasting. Body height and weight was measured in light clothing and without wearing shoes using JENIS (DS-103M, Dong San Jenix, Seoul, Korea) and Body composition was measured by Inbody 720 (Inbody 720, Inbody, Seoul, Korea) to confirm the BW, fat free mass (FFM), body fat mass (BFM), body mass index (BMI) and percent body fat (%BF)
Muscular strength and endurance assessments
The physical strength was measured by handgrip strength and back strength tests. The handgrip strength (T.K.K 5401, Tachometer, Takei, Tokyo, Japan) was measured twice at left and right sides. The back extension strength (T.K.K 5102, Takei) is important in core stability and it was measured twice. We recorded at the highest value in the test. All subjects took a rest for 3 min after 5 times of preliminary exercise and then maximal muscle strength was measured. To investigate the muscular endurance capacity, the sit-up (ST-110, Seed Tech, Seoul, Korea) was performed by lying on the floor and bending knees for 60 sec.
Flexibility and cardiorespiratory endurance assessment
Sit-and-reach (T.K.K 5403, Takei) test was performed by sitting on the floor with legs stretched out straight ahead, and subjects reaches forward along the measuring line as far as possible. We recorded at the highest value in the test. To examine that cardiorespiratory endurance capacity, 1,600-m running test was performed on the track (4×400-m track) and the total time to complete the test is recorded in minutes and seconds.
Blood concentration of lipid and adiponectin
To investigate blood concentration of TC, TG, HDL-C, LDL-C, and adiponectin. the venous blood samples were collected following a 12-hour overnight fast and then stored the centrifuged samples in a −80°. TC, TG, HDL-C, and LDL-C were analyzed by Enzymatic Colorimetric Assay, and adiponectin were examined by human adiponectin enzyme-linked immunosorbent assay kit (Abcam, Boston, MA, USA).
Statistical analysis
PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA) was used to determine the effect of resistance circuit training in obese college students. To confirm the main effect, we used a two-way repeated measures analysis of variance. If there was a significant interaction effect, an independent t-test between groups or a paired t-test between times was applied. All values are expressed as mean± standard deviation. P<0.05 was considered significant.
RESULTS
Resistance circuit training regulated the body composition in obese men
Changes of the body composition including BW, FFM, BFM, BMI, and %BF in obese college students were investigated at 2 days before and/or after the experiment. As shown in Table 3, BW (F=8.986, P<0.008) showed interaction effect between the two groups. RCG had a significant decrease of BFM (F=15.921, P<0.001), BMI (F=9.491, P<0.006), and %BF (F=16.981, P< 0.001) compared to those in SG, while FFM (F=0.030, P<0.865) showed no significant interaction effect between the two groups.

Changes of body composition
Resistance circuit training regulated the health-related physical fitness in obese men
Physical fitness may be defined as the ability to achieve physical activity and it is one of the powerful factors in assessing healthy living in adolescent, adult, and the elderly (Ganley et al., 2011; Liao et al., 2013; Ortega et al., 2008). Health-related physical fitness is composed of the body composition, grip strength, back strength, muscular endurance, flexibility and cardiorespiratory endurance (Ganley et al., 2011). As shown in Table 4, RCG had a significant difference of all health-related physical fitness such as the left grip strength (F=49.412, P<0.001), right grip strength (F=29.074, P<0.001), back strength (F=83.494, P<0.001), sit-up (F=47.964, P<0.001), sit-and reach (F=43.553, P<0.001), and 1,600-m running (F=18.278, P<0.001) compared to those in SG.
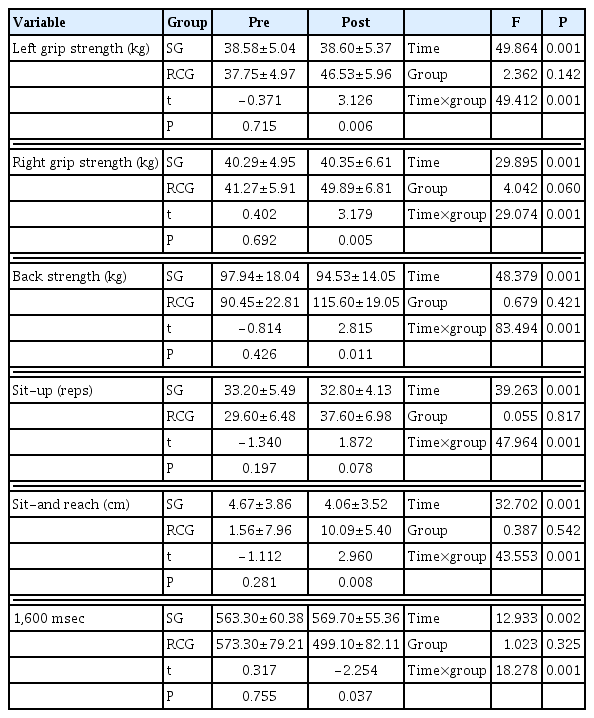
Changes of health-related physical fitness
Resistance circuit training regulated the levels of blood lipid and adiponectin in obese men
The values of plasma lipid profile and adiponectin in SG and RCG are shown in Table 5, and we confirmed significant interaction in blood concentration of TC, HDL-C, LDL-C, TG, and adiponectin between the two groups. As shown in Table 5, RCG had a significant alteration of TC (F=7.681, P<0.013), HDL-C (F= 7.216, P<0.015), LDL-C (F=7.242, P<0.015), and TG (F=30.270, P<0.001) compared to those in SG, while adiponectin (F=0.348, P<0.563) showed no significant interaction effect between the two groups.
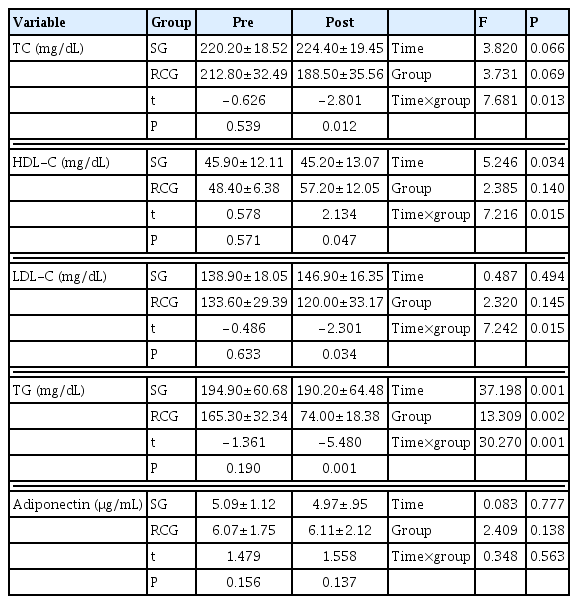
Changes of the levels of blood lipid and adiponectin
DISCUSSION
Obesity is one of the important indicators that can regulate healthy living and quality of life in modern people, and regular physical activity is known to play a decisive role in BW and %BF loss (Golbidi and Laher, 2014). Thus, we analyzed resistance circuit training for improving the physical fitness and physiological problems in obese male college students.
Health-related physical fitness is defined as the body capacity to work physical activities into daily living with efficiency, and it is made up of five fitness such as body composition, muscular strength, muscular endurance, flexibility, and cardiovascular endurance. Of these, lowering cardiovascular endurance and muscular functions in obese people have been reported to lead to cardiopulmonary disease, metabolic syndrome, skeletal disorder, and mental problem (Liao et al., 2013; Ortega et al., 2008). First of all, we investigated the body composition between the two groups, and confirmed that resistance circuit training for 12 weeks resulted in a significant decrease of BW, BFM, %BF, and BMI compared to those in SG. In previous studies related to the body composition in obesity, a short term high-intensity circuit training significantly decreased the percent fat tissue and increased the percent lean tissue by 3.6% and 2%, respectively (Miller et al., 2014). In addition, circuit weight training downregulated total body mass, fat body mass, and BMI, but there was no change in lean body mass in individuals with obesity (Ferreira et al., 2010). These findings in previous and present studies support the reasons why obese male college students should work out regularly for alternating the body composition.
In addition to the body composition, all other physical fitness including muscular strength, muscular endurance, flexibility, and cardiovascular endurance showed a significant interaction between RCG and SG. Muscular strength refers to the amount of force generated by a specific muscle, but muscular endurance is the ability of a specific muscle to sustain external loads. For the measurement of two physical fitness, grip strength and back strength tests are mainly applied to muscular strength, and sit-up tests are applied to muscular endurance. Cardiovascular endurance is a critical factor that reduce the risk of developing various metabolic disease and it is improved by regular aerobic exercise. And as a measurement method, the 1,600-m running test has been generally used. In previous studies, Oliveira-Junior et al. (2021) exhibited that combined circuit weight training for 12 weeks significantly improved maximum oxygen uptake, and flexibility rather than muscular strength and endurance in obese sedentary workers as well as Sperlich et al. (2017) verified that high-intensity circuit training enhanced muscular strength of upper and lower bodies, and improved muscular endurance through performing push-up, burpees, one-leg squats and 30 sec skipping tests compared to those in high-volume low-intensity circuit training. These data provide evidence that resistance circuit training can improve health-related physical fitness via muscle hypertrophy, motor unit activation, increase of capillary density and actin-myosin interaction in skeletal muscle (Elgueta-Cancino et al., 2022; Ramos-Campo et al., 2021).
Lipids are fat-like substances observed in the blood and body tissue, and it has been known as a risk factor to predict cardiovascular diseases (Ottosson et al., 2021). In obese people, an increase in BFM not only up-regulate blood concentration of TC and LDL-C, but also down-regulate HDL-C level. However, it is reported that BW and BFM reduction through regular exercise participation can improve these blood levels of lipid profile (Katzmarzyk et al., 2001). We investigated plasma concentration of TC, TG, HDL-C, and LDL-C after resistance circuit training for 12 weeks, and confirmed positive changes in all lipid profiles in RCG compared to those in SG. Previous studies analyzing exercise and blood lipid in obese people have emphasized that regular exercise considering intensity, frequency and time reduced blood concentration of TC, TG and LDL-C that lead to arteriosclerosis, and increased HDL-C level for vascular improvement (Doewes et al., 2022; Magkos et al., 2006; Omar et al., 2021). These results implicate that resistance circuit training may be one of the therapeutic methods for attenuating risk factors of cardiovascular disease in obese people.
Adiponectin is a protein hormone secreted by adipocytes to help with insulin sensitivity and inflammation (Ahima, 2006), regulating glucose metabolism in the skeletal muscle and adipocyte by activation of phosphorylated AMP-activated protein kinase and proliferator-activated receptors. Obese people have a lower plasma concentration of adiponectin than normal people, and reduction of BW and BFM increase adiponectin levels in the blood (Yamauchi et al., 2003). However, in the present study, although 12-week resistance circuit training in obese male college students downregulated BW and BFM, plasma concentration of adiponectin did not show a significant interaction effect between RCG and SG. Considering that many previous studies on exercise and adiponectin mechanism in obesity don’t produce consistent research results, it is necessary to think deeply about whether exercise regulates the blood level of adiponectin in obese people.
Given these findings reported in present study, resistance circuit training for 12 weeks would be effective in attenuating the body composition and blood lipid profile.
In conclusion, the present study suggests a main information that resistance circuit training may be a therapeutic approach to improve quality of life in obese male college students through regulation of physiological factors and physical fitness.
ACKNOWLEDGMENTS
This research was supported by the 2021 scientific promotion program funded by Jeju National University.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported