Relationship between strength training and shoulder pain in male and female water polo players
Article information

Abstract
The objective of this study was to assess the effect of two different strength-training methods on both male and female water polo players’ performance and shoulder pain. The players were randomly allocated to a maximum strength (MS: 14 males, 8 females) or power strength (PS: 13 males, 8 females) training group. Before and after the intervention, we assessed player’s anthropometric characteristics, shoulder internal and external rotation strength, hand grip strength, upper body strength, countermovement jump height, throwing velocity, swimming speed, shoulder pain on a visual analogue scale (VAS), wellness, and rate of perceived exertion per session. We observed no significant improvement (P<0.05) in specific skills but enhancement in hand grip strength in male players. In female players in the MS group, throwing speed and bench press weight decreased significantly (P<0.05). Shoulder external rotation strength at 240°/sec in male MS group players and shoulder external rotation strength at 60°/sec in female PS group players decreased significantly (P<0.05). In addition, from the first to the last week, shoulder pain increased significantly (P<0.05) in all players. Inverse correlations (P<0.05) were found between VAS and shoulder rotation strength in males in the PS group, and between wellness and shoulder internal rotation strength in men in the MS group and women in the PS group. We found that both MS and PS training did not enhance performance and increased shoulder pain in male and female water polo players.
INTRODUCTION
Water polo is a physically demanding water-based contact sport that requires intense bursts of sprint swimming and frequent changes of direction. Because water polo training includes swimming, knowledge of shoulder pain and injury risk for competitive swimmers can be applied to water polo players (Hams et al., 2019a). However, water polo also requires unique techniques as well as head-up swimming characterized by shorter strokes and a higher elbow position, with a reduction in body roll and increase in shoulder internal rotation (IR) and abduction (Colville and Markman, 1999). Furthermore, water polo requires ball throwing, repetitive passing, and shooting, which involve shoulder abduction and maximal external rotation (ER) at high speed (Melchiorri et al., 2011). In most water-based launches, there is a greater demand on the musculature of the shoulder (Yaghoubi et al., 2014), increasing the load and risk of injury.
Repetitive throwing is associated with shoulder injury, with the rotator cuff tendons most frequently injured (Dutton et al., 2019). In water polo players, biomechanical factors and specific requirements for throwing a ball while treading water tend to promote greater IR than ER shoulder strength (Barrenetxea-Garcia et al., 2019), which is associated with a high risk of imbalances of the shoulder and other problems (Clarsen et al., 2014). Although biomechanical changes in the shoulder do not always lead to pain (Beitzel et al., 2016), they are a source of clinically meaningful changes in water polo players, such as proprioceptive deficits (Mota and Ribeiro, 2012), patterns in forward scapular posture, and alterations in scapular muscle activity (Whiteley et al., 2012). Shoulder injuries among water polo players range from 25% to 80%, and this reflects the magnitude of the phenomenon (Miller et al., 2018). In addition, injuries that do not result in loss of playing time are not usually taken into account in large-scale studies of water polo players, underestimating the burden of shoulder pain (Girdwood and Webster, 2021). Although the nature of the problem remains unclear, risk factors include shooting volume, restricted range of motion, scapular dyskinesis, strength imbalance, proprioceptive deficit, and altered throwing kinematics (Miller et al., 2018). Injury rates also differ with performance level (i.e., elite vs. college), age range (senior vs. junior), and sex (Hams et al., 2019a).
During last decade, athletes of several disciplines have included strength training in their routines, including those in disciplines that traditionally have not utilized it, such as endurance athletes or cyclists (Balsalobre-Fernández et al., 2016; Rønnestad and Mujika, 2014). The development of muscular strength is a multifaced process influenced by a combination of structural and neural elements, encompassing aspects such as muscle cross-sectional area (CSA), architectural composition, musculotendinous rigidity, motor unit recruitment, rate coding, motor synchronization, and neuromuscular inhibition (Suchomel et al., 2018). Engaging in strength training yields several notable benefits, including enhancements in anaerobic power and maximal strength (García-Pallarés and Izquierdo, 2011), fostering strength gains via muscle hypertrophy (Izquierdo et al., 2004), and promoting heightened intramuscular and intermuscular innervation (Häkkinen et al., 2000). Furthermore, it amplifies the body’s capacity to respond effectively to the physical demands inherent in various forms of physical activity (Sáez de Villarreal et al., 2014). On a physiological level, the generation of force hinges upon the mechanical tension generated by muscle fibres in response to nerve impulses. These impulses trigger contractions within the relevant muscle groups required for a given action (González et al., 2023).
There is also strong evidence supporting the use of strength training in throwing sports such as handball (Bragazzi et al., 2020) and in swimming (Wirth et al., 2022). Given that water polo combines characteristics of the aforementioned sports, it seems logical to think that strength training should became a key factor for player’s success. However, there is a paucity of data on the value of strength training in male and female water polo players. Physical performance can be defined as the quantitative assessment of an athlete’s efforts and physical capabilities dedicated to achieving specific performance related goals and objectives within a defined timeframe. The current evidence shows that strength and high-intensity training led to improved swimming velocity and throwing performance in male water polo players (Sáez de Villarreal et al., 2014; Veliz et al., 2014). In female water polo players, no studies have evaluated the benefits of strength training, although strong female elite players exhibit an advantage during competitions (D’Auria and Gabbett, 2008; Veliz et al., 2015). This finding suggests that strength training may also benefit female players. On the other hand, although strength training can improve performance, overtraining can be detrimental.
Prolonged and demanding use of the rotator cuff leads to thickening and chronic overload (Michener et al., 2015), thereby increasing the frequency of homalgia episodes (Williams and Kelley, 2000). The symptoms of homalgia can range from mild discomfort to severe pain, which can be assessed by the visual analogue scale (VAS) (Macías-Hernández et al., 2020). It has been found that 74% of shoulder pain in water polo players could be attributed to the cumulative volume of throws and reduced resting periods between activities (Wheeler et al., 2013). Additionally, the extensive range of movements involved in swimming, both with and without the ball, has been shown to induce greater fatigue in the rotator cuff muscles (Colville and Markman, 1999). In particular, female players have a higher risk of shoulder injury from training overload than do male players (Asker et al., 2018), suggesting that training optimization is different in men and women. The objective of this research was to ascertain the relationship between strength training, performance, and shoulder pain in male and female water polo players. To provide empiric evidence on the value of strength training in male and female water polo players, we assessed the effect of two specific training methods: maximum strength (MS) and power strength (PS) were chosen as these are the most common methodologies applied by the national coaches. The findings of this investigation will inform the development of training programs targeted at maximizing players’ athletic performance.
MATERIALS AND METHODS
Design
Participants were randomly assigned by means of sealed opaque allocated into a MS (14 males, 8 females) or PS (13 males, 8 females) training group. MS training consisted of loads of 70%–90% 1 repetition maximum (1RM) performed at a medium-to-slow speed, while PS training consisted of loads of 50%–70% 1RM performed at a fast speed. Both groups included two specific strength sessions in their weekly programs. One of the women’s strength sessions for both MS and PS groups was based on compensatory exercises. Participant training sessions are described in Table 1. All participants completed a 12-week training program, trained 4 times a week for approximately 2 hr each session, and played a match every weekend. Strength training was tailored for each participant based on their MS. Written informed consent was obtained from players and parents or legal guardians in the case of participants under 18 years of age. This study was fully approved by the Human Research Ethics Committee of the University of the Basque Country (Ref. M10/290) and were adjusted to the Code of Ethics of the World Medical Association (Declaration of Helsinki, Fortaleza actualization, 2013). This trial was registered with the Australian and New Zealand Clinical Trials Registry (Registration number: ACTRN12618001724268).
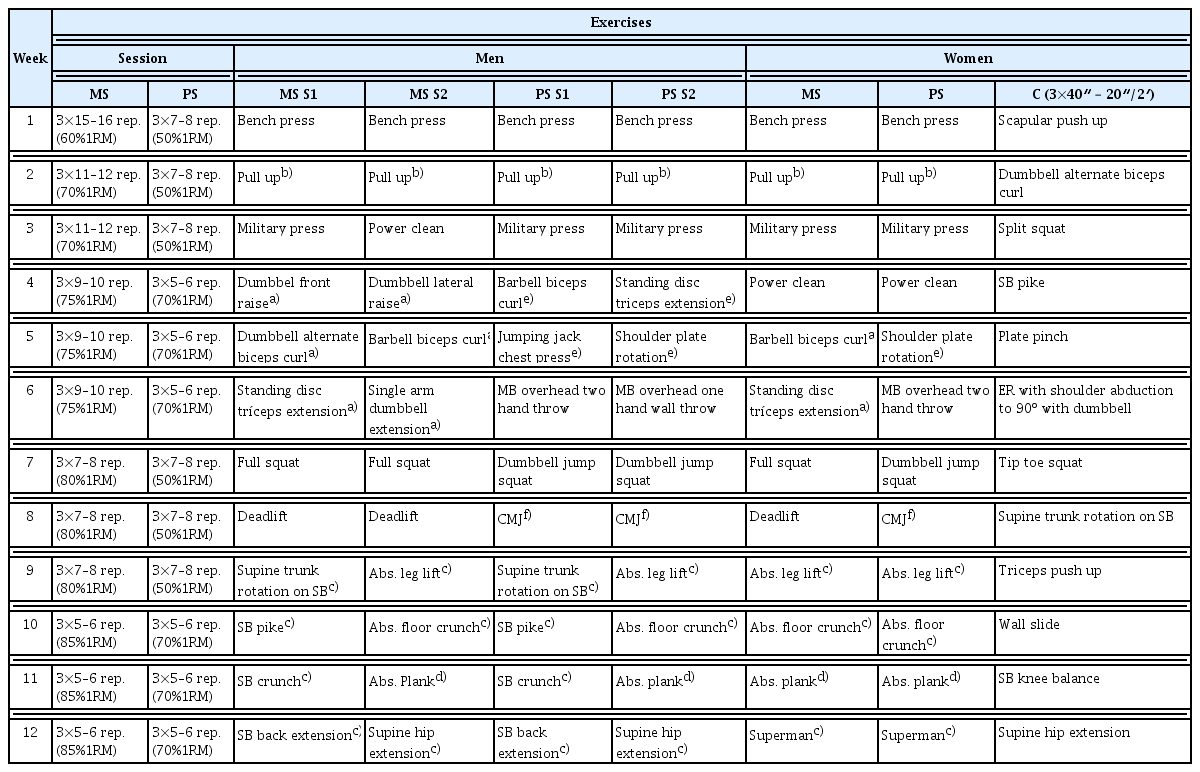
Training program for male and female players
Subjects
Male and female water polo players from the Leioa Waterpolo Club in Spain were invited to take part in the study. Inclusion criteria were five or more years of water polo experience, no history of shoulder pain or upper arm injuries in the previous year and completed 80% of the training sessions. Exclusion criteria were players with surgical history in shoulder, recent traumatic shoulder injury, cervicobrachialgia or other limitation of the joint range under rehabilitation treatment. We recruited 27 males (average age: 19.7±5.8 years; height: 176.7±6.7 cm; body mass: 76.5± 14.6 kg) and 16 females (average age: 19.5±6.1 years; body height: 165.6±6.4 cm; body mass: 61.5±6.2 kg).
Anthropometry
Each player was weighed (kg) using digital scales (HD–314 W, Tanita, Arlington Heights, Chicago, IL, USA), and stature and arm span were measured (cm) with a measuring rod (T-226 Marsden, Rotherham, UK) and anthropometric tape (W606PM Lufkin, Cooper Industries, Lexington, KY, USA) respectively. Body mass index was calculated as weight (kg)/height (m2). We collected subscapular, triceps, biceps, iliac crest, supraspinal, abdominal, thigh, and calf skinfolds (mm) with calipers (Harpenden, London, UK); elbow, wrist, knee, and ankle diameters (cm) with bicondylar calipers (Holtain, Crymych, UK); and relaxed arm, arm in flexion and tension, waist, hip, thigh, and calf perimeters (cm) with a tape measure (Mannesmann, Mülheim an der Ruhr, Germany). All measurements were obtained by the same person, who was certified by the International Society for the Advancement of Kinanthropometry. Each measurement was obtained twice, and the mean was used for statistical analysis. Bone, muscle, and fat percentages were determined as described in Barrenetxea-Garcia et al. (2019).
Isokinetic muscle test
Participants laid supine on an isokinetic machine (Humac Norm, Computer Sports Medicine Inc., Stoughton, WI, USA) with the shoulder at 90º abduction. Range of movement was determined individually and was defined as an arch of physiological movement without major discomfort for the athlete. Corresponding tests were IR and ER at an angular velocity of either 60º/sec or 240º/sec. All were concentric contractions. Each test consisted of an initial warm-up, two sets of five repetitions each (with 20 sec of rest between the series), and 1 min of rest at the end of each test. Variables obtained by isokinetic assessment of the shoulder were IR and ER for peak torque (PT, measured in N·m). We also calculated PT using body weight (N·m.kg). Before the isokinetic tests, participants completed a standardized warm-up using PRO2 Sport Total Body ergonomics (SciFit, Tulsa, OK, USA). The warm-up lasted 3 min and was carried out under a load of 25 N and at an intensity of 40 repetitions per minute. Participants performed 3 sets of 15 repetitions of alternative IR, ER, and IR in 90º abduction, and ER in 90º abduction exercises in an EN-Tree P pulley (Enraf Nonius, Rotterdam, Netherlands) (Barrenetxea-Garcia et al., 2019).
Hand grip test
A hand grip test was performed with a hydraulic hand dynamometer (Jamar, Anaheim, CA, USA). Participants remained with one arm parallel to the body in adduction and exerted maximum contraction for 5 sec. All athletes performed the test twice for each hand, and the highest value obtained in each hand was recorded.
Bench press test
Participants lay in a supine position with their back and buttocks resting on the bench and feet on the ground, holding a bar with a prone grip to detach and raise it from supports by extending the arms to reach the start position with the elbows extended to chest height. Before the test, participants performed a standardized warm-up of a series of 10 repetitions with loads of 40 to 60% of their perceived 1RM (Sáez de Villarreal et al., 2014). The test consisted of five series of maximum repetitions, in ascending progression, with 2 min of rest between each.
Countermovement jump test
The countermovement jump test (CMJ) was performed using an infrared beam system (Optojump, Microgate, Bolzano, Italy) to measure flight and contact times. Jump height was determined from the flight time using a standard calculation. Three trials were completed with a 2-min rest between trials, and the mean was recorded (Veliz et al., 2015).
Throwing velocity test
In the swimming pool participants threw a ball at a goalmouth as quickly and as accurately as possible from a distance of 5 m. The test consisted of three sets of three repetitions, with 15 sec of rest between throws, and 1 min between sets. Measurement was carried out by Stalker SOLO radar (Plano City, TX, USA). Before the test, participants performed a standardized warm-up of 10 min of free swimming and 5 min of passes with an official ball (Sáez de Villarreal et al., 2014).
Swimming speed test
The swimming speed test was carried out in a competition pool with standard dimensions (25×12.5 m) with the objective of assessing how long each player took to swim 20 m at their maximum swimming speed. The measurement was performed with an electronic timing system (Casio HS-3V-1, Tokyo, Japan). Before the test, participants completed a standardized 15-min warm-up. Athletes were asked to adopt an upright position with their backs facing the direction they were going to swim and after a signal make a 180° turn and swim the established distance. The test consisted of three sets of one repetition at maximum speed, with a 5-min rest between sets. The best time was recorded (Veliz et al., 2014).
Wellness test
A questionnaire was distributed to participants based on the recommendations of Hooper and Mackinnon (Hooper and Mackinnon, 1995) to evaluate fatigue, sleep quality, general muscle pain, stress levels, and mood on a scale of 1 (poor) to 5 (excellent).
VAS
VAS measures the intensity of pain described by athletes and is widely validated in the follow-up of pain (Tashjian et al., 2009). It consists of a 10-cm horizontal line with descriptive expressions of images of faces responses orientated from the left (worst) to the right (best).
Rate of perceived exertion per session
Training loads for each training session were recorded using the methods described by Foster et al. (2001). This method calculates a total training load (arbitrary units, AU) by multiplying the rate of perceived exertion (RPE) by the length of the session. Each athlete rated the perceived intensity of the entire session using the RPE scale (from 0 to 10). Players were briefed on the correct use of the scales and the objectives of the study, before being familiarized with the procedures during field training sessions within the 2 weeks leading up to study commencement. Before and after the intervention, we assessed anthropometric characteristics, IR and ER shoulder strength, and performed other functional tests such as hand dynamometry, bench press, CMJ, throwing velocity, and swimming speed. In addition, wellness and RPE per session (sRPE) were assessed at the beginning and end of each training session, and VAS was assessed after each strength session. Isokinetic assessments, dynamometry tests, and warm-ups were carried out in a laboratory of the Faculty of Medicine and Nursing of the University of the Basque Country. Other tests were carried out in the sports center of the club. Sessions were held on weekdays beginning at 3:00 p.m. and ending at 8:00 p.m. (the same hour was assigned for each subject assigned in both pre and post assessments). During the intervention, participants performed strength sessions in individual rooms. Each session lasted 45–50 min, including time for warm-up and stretching. Water training (swimming and water-specific work), lasting 2 hr, took place in the swimming pool. Participants were supervised during each test and were instructed to maintain their usual eating habits as well as other routines for the duration of the study.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). The Shapiro–Wilk test was used to assess whether the data were normally distributed. The level of significance was set at P<0.05. Data are presented as mean±standard deviation and percentages. Differences between training groups were analysed using Student t-test (parametric variables) or Mann–Whitney U-test (nonparametric variables). The magnitude of interactions between the intervention time and the group was assessed as described by Cohen (1998) and interpreted as small (>0.01 and <0.06), moderate (≥0.06 and <0.14), or large (≥0.14). Differences between the first week and the last week, as well as percent changes (%), were analyzed using a paired Student’s t-test (parametric variables) or Wilcoxon test (nonparametric variables). The strength of association between muscle strength and test results were assessed by Pearson (parametric variables) or Spearman (nonparametric variables) correlation coefficients.
RESULTS
The results of functional tests for both male and female players are shown in Table 2. After the intervention, hand grip strength improved significantly in both groups of male players (P<0.05), but most notably in those in the MS group (P<0.001; large interaction). Changes in the other tests were not significant. In female players, hand grip strength overall improvement was not statistically significant. However, unlike the pattern observed in male players, hand grip improved more among female players in the PS than the MS group (P<0.05; large interaction). Remarkably, female players in the MS group performed more slowly in the throwing test (P<0.01; large interaction) and lost lifting capacity in the bench press test (P<0.05) after the intervention. The same trends were observed for female players in the PS group, but the changes were not significant.

Hand grip strength, swim sprint, throwing velocity, jump height, and bench press test performance by training type in male (n=27) and female (n=16) water polo players
Shoulder rotation force measurements before and after the intervention are shown in Table 3. Male players did not improve IR or ER strength after the intervention in either group. Furthermore, after the intervention, both groups of male players performed worse on the ER strength test at 240°/sec (P<0.01), especially in the MS group (P<0.001; large interaction). Female players in the MS group appeared to show a decrease in performance on all the isokinetic tests, but the changes were not significant. Female players in the PS group showed a significant decrease (P<0.05) in both ER and normalized ER strength at 60°/sec test (P<0.05; large interaction).
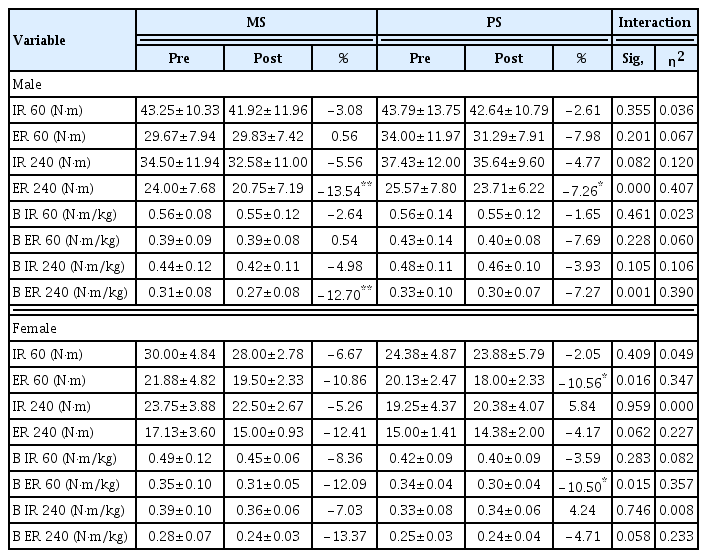
Isokinetic peak moment strength values by training type in male (n=27) and female (n=16) water polo players
The weekly sRPE, wellness, and shoulder pain rated on the VAS are presented in Figs. 1 and 2 for male and female players, respectively. In male players in the PS group, from the first to the last training session during the 12-week intervention, we observed significant (P<0.01) worsening in VAS, wellness, and sRPE, with relative changes of 7.44%, 20.18%, and 47.62%, respectively. A relative increase of 37.78% in VAS score (P<0.05) was also found in players in the MS group. Curiously, significant time and group interactions (P<0.001, large effect) were found in male players for the VAS, wellness, and sRPE scores. In female players, from the first to the last week, VAS score increased significantly (P<0.01, large effect), with relative changes of 80.65% and 97.14% in the MS and PS groups, respectively.
Weekly rate of perceived exertion per session, wellness and shoulder pain rated on the visual analogue scale in male water polo players during the training program. MS, maximum strength training; PS, power strength training. *P<0.05, MS group, week 1st vs. 12. †P<0.05, ††P<0.01, PS group week, 1st vs. 12. ‡‡P<0.01, ‡‡‡P<0.001, time and group interactions.

Weekly rate of perceived exertion per session, wellness and shoulder pain rated on the visual analogue scale in female water polo players during the training program. MS, maximum strength training; PS, power strength training. *P<0.05, MS group, week 1st vs. 12. †P<0.05, PS group week, 1st vs. 12. ‡‡P<0.01, time and group interactions.
Correlation coefficients between VAS, wellness, sRPE, and shoulder IR and ER strength measured with the isokinetic system for both male and female players are shown in Table 4. In male players in the MS group, IR strength at 240°/sec correlated negatively with wellness score (r=−0.825, P<0.01) and positively with sRPE (r=0.737, P<0.05). Similarly, significant correlations were found between the IR BW strength test at 240°/sec and wellness score (r=−0.646, P<0.05) as well as sRPE (r=0.623, P<0.05). Session RPE was also correlated with the ER strength test at 60°/sec (r= 0.636, P<0.05). In male players in the PS group, sRPE correlated with the IR strength test at 60°/sec (r=0.652, P<0.05) and at 240°/sec (r=0.626, P<0.05), as well as with the ER strength test at 60°/sec (r=0.732, P<0.01) and at 240°/sec (r=0.608, P<0.05). Further, shoulder pain correlated negatively with the normalized IR strength test at 60°/sec (r=−0.638, P<0.05) and at 240°/sec (r=−0.668, P<0.01), and with the normalized ER strength test at 60°/sec (r=−0.546, P<0.05) and at 240°/sec (r=−0.688, P<0.01) in the male PS group. In female players, significant correlations were found only for the PS group in which wellness scores were negatively correlated with the IR strength test at 60°/sec (r=−0.876, P<0.001) and at 240°/sec (r=−0.954, P<0.001), as well as with normalized IR at 60°/sec (r=−0.763, P<0.05) and at 240°/sec (r=−0.852, P<0.01). A significant correlation between shoulder pain and IR at 240°/sec was found in female PS participants (r= 0.748, P<0.05).

Pearson’s correlations between wellness, sRPE, VAS scores and isokinetic peak moment strength by training type in male (n=27) and female (n=16) water polo players
DISCUSSION
This study evaluated the effect of two different training methods on shoulder pain and performance among water polo players. According to Furrer et al. (2023), optimal training strategies should not only comprise personalized planning but should also integrate adequate consideration of recovery and injury prevention. From this point of view, this manuscript contributes to an innovate perspective that integrates strength training and pain assessment. The training intensity could be the factor determining an athlete’s adaptability, and thus, it seems key for enhancing performance and reducing risk of injuries. In this sense, there is a scientific debate about whether training volume or training intensity promotes the greatest adaptation in skeletal muscle. While MacInnis et al. (2019) hypothesized that the biochemical mechanisms that promote mitochondrial biogenesis are controlled by exercise intensity, Bishop et al. (2019) published that there was no evidence that exercise intensity is more important than exercise volume to promote increases in mitochondrial content. Recent publications in this sport suggest that there may be a positive relationship between strength training and performance in this sport; however, the small number of studies and their heterogeneity have made it difficult to translate findings into best practices. Botonis et al. (2016) demonstrated that two protocols of high-intensity training in combination with MS training enhanced swimming endurance and upper limb strength of elite male players. Similarly, Sáez de Villarreal et al. (2014) reported that performance, particularly swimming agility, improved in elite male players after an in-water strength protocol. Furthermore, significant improvements in throwing performance were demonstrated by Veliz et al. (2014).
However, only one study (Veliz et al., 2015) focused on female player strength training, finding improvements in water polo-specific skills. The female protocol focused only on lower limb strength. Therefore, there is a lack of definitive studies evaluating upper body strength training programs and their impact on water polo players of both sexes. Ours is the first study to compare the effects of MS and PS training methods on the performance of both male and female players. In male players in both the MS and PS groups, we did not find any significant changes in specific skills except for enhancement of hand grip strength, which was improved in the MS group. In the female players, hand grip strength increased in the PS group. The increase in hand grip strength may result from the use of the bars during both the MS and PS training programs. Differences between sexes was an unexpected finding, which may result from male players in the MS group using heavier dumbbells, while female players in the PS group used small-size medicine balls in their routines.
It is worth nothing that throwing speed and bench press strength decreased significantly among female players in the MS group. Similarly, isokinetic testing did not reveal improvements in the shoulder rotation forces for male or female players, and the values were lower than these found in previous studies with similar samples (Barrenetxea-Garcia et al., 2019). Spieszny and Zubik (2018) found in handball that specific strength training does not improve throwing performance. In the same line, Herman et al. (2008) hypothesized that the mere fact of increasing the muscle strength may not produce biomechanical changes, but loss of strength could affect it negatively. The individual’s responses to training should also be considered. As has been previously described, considerable evidence exists to distinguish elite athletes from less well-performing athletes with respect to both genetic factors and training histories (Tucker and Collins, 2012). In fact, few gene variants have been found in the phenotype of power athletes (Ahmetov et al., 2016). In resume, genetic factors and training background could also contribute to explain the lack of improvement of the performance of some of our players. In any case, the relatively small size of our training groups and the nature of the study would have made extremely difficult look into these topics.
Traditionally, strength training is not considered a contributor to shoulder pain in water polo players. However, pain is a particularly difficult variable to assess. It is worth nothing that strength training contributes notably to the phenomenon called “muscle memory” which is based on motor learning, intra- and intermuscular coordination, previous experience of body perception, resilience to give into pain and fatigue, and anticipation of exertion (Snijders et al., 2020). While most coaches incorporate strength training into their regiments under the assumption that it has a beneficial effect on players’ performance, they probably cannot ascertain its relationship with the pain. In this sense, athletes encounter varying degrees of painful stimuli. While some pain may result from muscle developmental due to repeated contractions (O’Connor and Cook, 2001), other factors such as increased internal pressure, tissue deformation or the accumulation of metabolites may contribute to exercise-induced pain (O’Connor and Cook, 1999).
In addition, experiences athletes tolerate more pain than novel ones, particularly in sports with higher levels of contact (O’Farrell et al., 2022). As the participants of this study were experienced players, we assume that they are used to certain levels of pain as a part of their routine. However, our results showed that PS and MS training could also contribute to worsening shoulder pain and, consequently, reduce performance. Indeed, we observed an increase in shoulder pain in both male and female players over the course of the intervention. According to previous publications, values over 3 points on the VAS are considered clinically meaningful in shoulder pathology (Tashjian et al., 2009). In our study, male players had VAS scores over 3 points starting in the first week, and female players exceeded this threshold by the third week of strength training. In both sexes, an upward trend was observed in VAS scores, with significant increase in pain from the first to the last week. In addition, we also observed a decrease in rotational shoulder strength after the intervention, which could also increase the risk of injury (Hams et al., 2019b). Curiously, male players in the MS group and female players in the PS group had the highest pain scores and greatest loss of strength compared to their peers of the same sex. Although the inhibitory effect of pain on sport performance has been previously described in other sports (O’Connor and Cook, 1999), to our knowledge, this is the first description of the phenomenon in water polo players. Besides, PS work shows less pain perception. However, MS work is necessary. No single exclusive training method can achieve the range of adaptations required for strength and related force-time characteristics (Suchomel et al., 2018). Therefore, combining heavy and light loads could produce the desired strength adaptations (Suchomel et al., 2018). However, this combination should be investigated in future research.
An insufficient recovery process may also negatively influence player performance and provoke shoulder pain. In line with Wheeler et al. (2013), who demonstrated that the combination of increased volume of sport-specific skills training (i.e., throwing) and less rest time between training sessions can increase shoulder pain, we also found a negative correlation between sRPE and wellness scores. Briefly, the greater the load of strength work, the greater the shoulder pain, which also negatively affects the perception of accumulated fatigue. A direct association has been observed between increased muscle force production and increased pain intensity (Cabral et al., 2023). Besides, the accumulation of pain can increase the effort sense (Hollander et al., 2008). Therefore, recovery after exercise is an essential part of sports performance, and its evaluation and monitoring are necessary (Calleja-González et al., 2018). We also hypothesize that the combination of a ceiling effect and fatigue accumulated through the season negatively influences the performance of players, and could explain the above-mentioned lack of improvements in the shoulder rotation forces for male or female players. Additional results would need to be added in future research, for example, measuring the CSA of the pectoralis major and biceps brachii muscles by ultrasound.
A limitation of this study is the relatively small size of the sample. In comparison with other sports more popular in Spain, there are relatively few elite water polo players. We also recognize that the matches during the league may have affected the measurements. In addition, the lack of a control group limits the comparability of the findings, but due to the nature of this research, it seemed unethical to create a subgroup that did no strength training. It would be interesting to compare the results with players from other levels (international, elite and elite) and contexts.
In summary, the study showed that strength training enhances shoulder pain, which could potentially negatively influence water polo player performance. Shoulder pain occurred when the training was based on MS for men and on PS for women. This sex difference should be considered in training program design. In addition, the volume of training and perceived fatigue should also be controlled. We suggest that coaches and technical staff of water polo teams as well as other sports involving throwing include regular measures of shoulder pain self-reporting and perceived fatigue.
ACKNOWLEDGMENTS
We express sincere gratitude to the parents and children who agreed to participate in this research and acknowledge the collaboration of the water polo club Leioa Waterpolo. The authors received no financial support for this article.
Notes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.